- 01
- Why CABGRationale + evidence
- 02
- What operationTargets + planning context
- 03
- What to askGaps + next questions
Your Incision Should Be Your Decision™
Bypass surgery second opinion
A cardiac surgeon and cardiologist independently review your complete record, confer, and co-sign one patient-facing report—clarifying why CABG was proposed, what the anatomy shows, what the operation involves, and what still deserves a question.
Direct-pay service · Live physician consultation is optional and costs extra · No referral or travel required

Not a generic answer about bypass. A case-specific map built from your complete record.
Explore the sample reportThe decision before consent
“You need bypass” names a procedure. It does not explain the full reasoning, the planned operation, the limits of the workup, or the trade-offs that matter to you.
The report connects symptoms, testing, coronary angiography, prior treatment, heart function, and the treating team’s rationale—without treating “you need bypass” as the whole explanation.
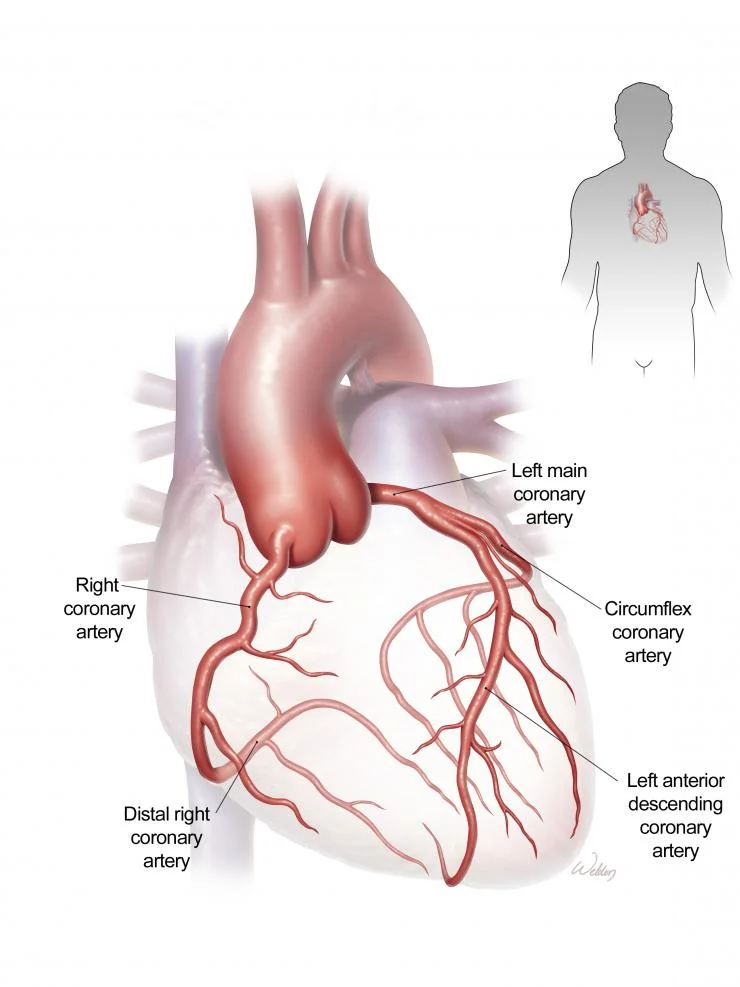
Left-main or multivessel disease, lesion location, calcification, chronic occlusions, distal targets, prior stents, and anatomic complexity can all shape the discussion.
The number and location of grafts, potential conduits, on-pump or off-pump context, other procedures, and unresolved planning questions deserve to be understandable before consent.
Missing images, incomplete testing, uncertain targets, medication issues, organ function, frailty, or another reasonable treatment path may create questions for the treating team.
Your anatomy, not a generic diagram
The report connects the cath images, heart function, prior treatment, other health conditions, and patient priorities to the operation being proposed.
Which major vessels and branches are narrowed, where the disease begins and ends, and which areas of heart muscle may need improved blood flow.
The size and documented quality of vessels beyond a blockage, diffuse disease, calcification, and whether the available record supports the proposed graft targets.
Whether the left main, proximal LAD, circumflex, right coronary artery, or several territories are involved—and why that pattern matters to the proposed strategy.
Ejection fraction, wall-motion findings, heart-failure symptoms, ischemia, valve disease, and whether another cardiac procedure is being considered at the same operation.
Previous stents, coronary interventions, bypass grafts, chest surgery, radiation, or vascular procedures that may affect the operative and alternative-treatment discussion.
Diabetes, kidney and lung function, prior stroke, peripheral vascular disease, bleeding history, frailty, medicines, functional status, and personal priorities.
The operation itself
The treating surgeon makes the operative decisions. The review gives you a readable framework for understanding the plan and asking better questions.
Which coronary targets are proposed and how the planned grafts relate to the angiogram.
Internal thoracic artery, radial artery, and saphenous vein considerations described as planning context—not a remote prescription.
CABG alone or CABG combined with a valve, aorta, rhythm, or other cardiac procedure.
Medication holds, missing workup, organ-function issues, blood management, rehabilitation, and discharge planning raised by the record.
Reasonable paths, not false equivalence
Not every path applies to every patient. The report explains the treating team’s proposed path, which alternatives deserve discussion, and where uncertainty or missing information remains.
The proposed operation organized around coronary targets, possible conduits, completeness of revascularization, operative context, recovery, and the documented reasons for surgery.
Stents may be relevant in selected anatomy. The report explains feasibility questions, completeness, contrast and bleeding considerations, antiplatelet therapy, durability, and why PCI may or may not have been proposed.
Medication and risk-factor treatment remain important with any strategy. In selected situations, the record may support asking whether medical therapy alone or further optimization deserves discussion.
When the record is incomplete, the report identifies the source images, functional testing, physiologic assessment, vascular testing, or clinical clarification that could make the next conversation more useful.
WHITEGLOVE Insights™
A patient-facing map of the bypass decision—built from the source record, reviewed from both sides of the Heart Team, and designed for your next conversation.
Download a sample reportWHITEGLOVE Insights™
Symptoms, diagnoses, heart function, medications, testing, angiography, prior procedures, and the treating team’s proposed plan—clearly attributed to the record.
A cardiac surgeon and cardiologist independently review the same complete record, confer, and co-sign one patient-facing report.
Relevant professional guidance and published evidence placed beside the details that make them applicable—or limited—in your case.
STS PROM, EuroSCORE II, and AATS considered separately when applicable, with inputs, missing variables, model limits, and clinical context made visible.
A patient-facing map connects the important lesions and territories in the record to the reason bypass was proposed.
Targets, possible conduit strategy, combined procedures, medication questions, and perioperative issues organized for discussion with the treating surgeon.
Surgical, catheter-based, medical, or information-first paths raised by the record compared without declaring them equivalent or selecting treatment.
Missing imaging, testing, documentation, or unresolved issues converted into a concise list for the next treating-team conversation.
Procedure-specific experience, public outcomes when comparable, team resources, geography, and practical transfer considerations organized without implying affiliation.
The concerns that matter to you and your family gathered in patient-facing language so they do not disappear during a high-stakes conversation.
No false completeness
A confident answer built on an incomplete record is not clarity. Required source images and records are confirmed before the 24-hour review window starts.
The actual coronary angiogram can show details that a written report cannot fully communicate. Source imaging is required when it is material to the review.
Valve findings, ejection fraction, wall motion, pulmonary pressures, and other cardiac findings can change the scope and context of surgery.
The clinic note, planned grafts or targets when documented, other proposed procedures, urgency, alternatives discussed, and the center where surgery is planned.
Age, laboratory values, organ function, functional status, prior procedures, urgency, and other variables needed for an applicable estimate—without inventing missing data.
When relevant, prior harvests, arm or leg history, vascular disease, and any documented testing that may inform—but does not remotely determine—conduit planning.
Recovery, work and caregiving, medication burden, travel, rehabilitation, transfusion concerns, durability, and the outcomes that matter most to you.
How it works
You bring the question. WHITEGLOVEMD helps complete the record, convenes the WHITEGLOVE Heart Team, and makes the analysis usable.
Choose the $495 written review when ready, or request a complimentary orientation call first. No referral or travel is required.
Upload what you have. With authorization, the records team can help identify and gather the catheterization images, reports, notes, echocardiogram, testing, labs, and proposed plan required for review.
A cardiac surgeon and cardiologist examine the same complete record from their respective perspectives, then confer on the final analysis.
Your WHITEGLOVE Insights™ report is delivered within 24 hours only after all records and imaging required for the review are received and confirmed complete.
Clinical rigor
Guidelines, published evidence, and risk tools inform—but do not replace—physician judgment. Risk estimates are population based, depend on accurate inputs, have procedure-specific limits, and cannot predict an individual outcome with certainty.
Start with the written review
The co-signed written review is $495. A live physician consultation is optional, available through higher-tier services, and costs extra.
WHITEGLOVE Insights™
Written Heart Team reviewDirect-pay service. WHITEGLOVEMD does not submit insurance claims. No referral is required.
Bypass surgery second opinion FAQ
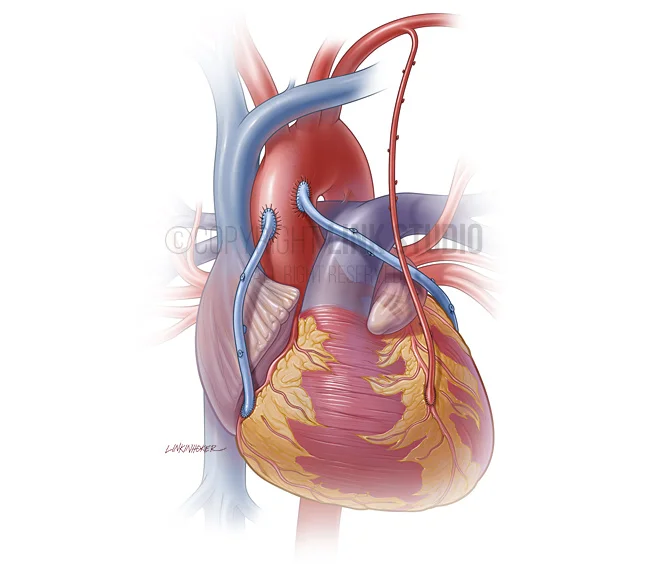
Coronary artery bypass grafting, or CABG, is an operation that uses blood vessels from the chest, arm, or leg to create new routes around narrowed or blocked coronary arteries. The exact operation depends on the coronary anatomy, proposed targets, conduit plan, heart function, other cardiac conditions, and patient circumstances. A webpage cannot determine whether CABG is appropriate for an individual.
A review can be useful when CABG has been proposed and you want to understand why, when anatomy or operative planning is complex, when bypass and stents are both being discussed, when another cardiac procedure may be added, when opinions differ, or when you want a clearer risk and workup discussion before consent. It should not delay urgent or time-sensitive care directed by your treating team.
No. WHITEGLOVEMD provides independent educational decision support and medical-record review. The report explains the documented rationale for CABG, the relevant anatomy and evidence, reasonable paths raised by the record, important uncertainties, and questions for your treating clinicians. It does not diagnose, determine candidacy, prescribe treatment, or replace your treating team.
The required record commonly includes source coronary angiography or catheterization images and the report, echocardiogram images and report when relevant, the cardiology and cardiac-surgery notes, the proposed operation, recent testing and laboratory results, medications, prior cardiac procedures, and pertinent medical history. The exact requirements depend on the case. The records team can help identify and gather what is missing with your authorization.
Yes, when those paths are relevant to the record. The report can organize CABG, PCI or stents, medical therapy, or a need for more information around the documented anatomy, symptoms, ischemia, diabetes, heart function, procedural considerations, durability, medication burden, and patient priorities. It does not assume the choices are interchangeable or that every option is feasible.
The report connects the proposed graft plan, when documented, to the coronary angiogram and target territories. It can identify questions about completeness, diffuse disease, target quality, or branches that may deserve discussion. A remote review does not direct the operation, select final graft targets, or replace the treating surgeon’s intraoperative judgment.
Yes, as educational operative-plan context when relevant. The report may explain internal thoracic artery, radial artery, and saphenous vein considerations in relation to the documented targets, age, comorbidities, prior procedures, and available records. It does not prescribe a conduit, assess a vessel remotely, or guarantee that a particular conduit can or should be used.
When applicable and supported by complete inputs, the review considers STS PROM, EuroSCORE II, and AATS separately and explains their outputs, missing variables, and limitations. These are population-based tools, not predictions of an individual outcome. Anatomy, frailty, organ function, combined procedures, surgeon judgment, and center resources may not be fully represented by a score.
The report audits the available workup against the documented operation and questions raised by the record. It may identify missing source imaging, reports, laboratory information, vascular or pulmonary evaluation, medication planning, or another unresolved item to discuss. It does not order tests or declare that every patient needs the same workup; the treating team decides what is clinically necessary.
The report can organize procedure-specific experience, publicly reported outcomes when available and comparable, program resources, geography, and practical transfer considerations. Public ratings and volume have limits and do not predict an individual result. WHITEGLOVEMD does not imply a hospital affiliation, endorse a program, or guarantee access or outcome.
A cardiac surgeon and cardiologist independently review the same complete record, then confer and co-sign one patient-facing WHITEGLOVE Insights™ report. The surgeon contributes operative, target, conduit, and perioperative context. The cardiologist contributes coronary imaging, heart function, medical therapy, catheter-based, and longitudinal context.
The WHITEGLOVE Insights™ written review is $495. A live physician consultation is optional, is available through higher-tier services, and costs extra. WHITEGLOVEMD is a direct-pay service and does not submit insurance claims. Current package details are shown before purchase.
The 24-hour review window begins only after every record and source image required for your case has been received and confirmed complete. Time spent identifying, requesting, transferring, or collecting missing records and imaging is outside that window.
No referral or travel is required for the written medical-record review. You may choose the written review alone or add an optional live physician consultation through a higher-tier service. Any testing, treatment, or in-person evaluation remains with your treating clinicians.
WHITEGLOVEMD does not provide emergency or urgent care. New or worsening chest pain, difficulty breathing, fainting, sweating with discomfort, sudden weakness, or other potentially urgent symptoms require immediate medical evaluation. Call 911 or follow your treating team’s emergency instructions. Do not wait for a second-opinion report.
Before the first incision
Start with the $495 co-signed written review. Add live physician time only if you want it.