Your Incision Should Be Your Decision™
CABG vs stents second opinion
CABG or stents?
Compare the whole decision.
A cardiac surgeon and cardiologist independently review your complete record, confer, and co-sign one patient-facing report—so anatomy, risk, recovery, durability, medications, and your priorities are considered together.
- 2
- independent specialists
- 1
- co-signed written report
- 24 hr
- after complete records
Direct-pay service · Live physician consultation is optional and costs extra · No referral or travel required
Case comparisonCABG · PCI · Whole record
WHITEGLOVE Heart TeamCardiac surgeon + cardiologist
Not a generic CABG-versus-PCI answer. A case-specific comparison built from your record.
Explore the sample reportThe decision in front of you
Four questions the comparison should make clearer.
The useful question is not whether CABG or PCI wins in the abstract. It is how each path fits your coronary anatomy, health, goals, and tolerance for different burdens.
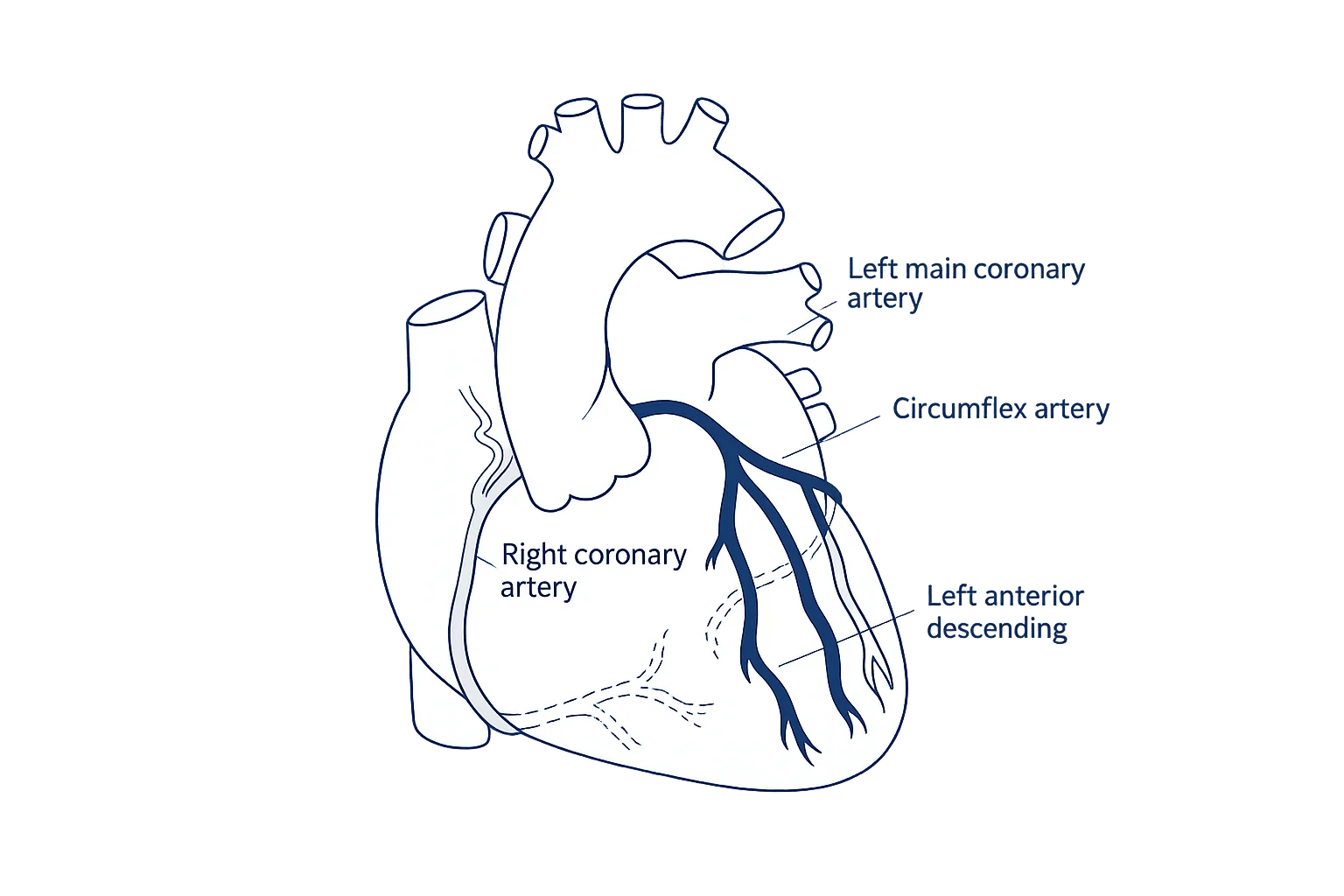
What does the coronary anatomy favor?
Left-main or multivessel disease, lesion location, calcification, chronic total occlusions, prior stents, and overall complexity can change how CABG and PCI are compared.
How do health factors change the trade-offs?
Diabetes, kidney or lung disease, prior stroke, bleeding risk, frailty, and left-ventricular function can affect both procedural risk and longer-term strategy.
What matters now—and years from now?
Recovery time, durability, the chance of repeat procedures, medication requirements, and completeness of revascularization deserve to be considered together.
Which priorities matter most to you?
Avoiding an operation, reducing repeat interventions, returning home sooner, treatment burden, and personal goals may carry different weight for different people.
Built from the whole record
What can change a CABG-versus-stents decision.
A lesion is only one part of the decision. The report organizes the clinical and practical variables that can materially change how the paths are understood.
Anatomy and complexity
Which vessels are narrowed, whether left-main or multivessel disease is present, lesion length and location, calcification, bifurcations, chronic occlusions, and the documented complexity of the pattern.
Diabetes and comorbidity
Diabetes, kidney function, lung disease, prior stroke, peripheral vascular disease, frailty, and other conditions that may influence procedural and longer-term considerations.
Left-ventricular function
Ejection fraction, regional wall motion, heart-failure symptoms, valve findings, and whether viability or other additional context appears relevant.
Surgical and PCI risk
Validated surgical-risk models when inputs are available, plus bleeding, vascular, kidney, stroke, and contrast-related considerations documented for a catheter-based procedure.
Durability and completeness
Whether either strategy can address the important territories, how repeat intervention may enter the discussion, and what the evidence says for a patient with this pattern.
Recovery, medicines, and priorities
Recovery expectations, antiplatelet therapy, adherence, planned procedures, work or caregiving responsibilities, and the outcomes that matter most to the patient.
Reasonable paths, in context
One record.
Several possible paths.
No automatic winner.
Not every path applies to every patient. The report explains which options deserve consideration, what the record says about each, and where important uncertainty remains.
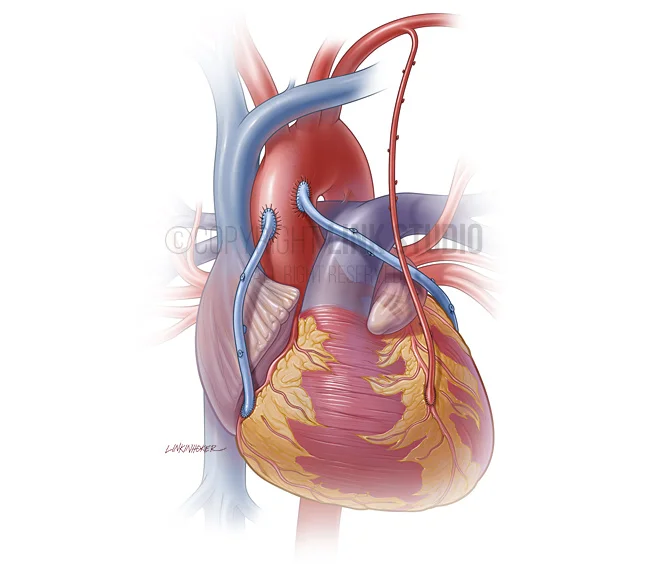
CABG
A surgical approach that can address several coronary territories in one operation. The review considers targets, conduit strategy, completeness, operative risk, recovery, and longer-term considerations.
PCI or stents
A catheter-based approach that may offer a shorter initial recovery. The review considers lesion complexity, completeness, contrast and bleeding considerations, antiplatelet therapy, and the possibility of later procedures.
Medical therapy
Medication and risk-factor management considered in relation to symptoms, ischemia, anatomy, disease stability, prior treatment, and why revascularization was proposed.
More information first
When the record does not support a clean comparison, the report identifies the imaging, functional testing, physiologic assessment, or clinical question that may help resolve uncertainty.
WHITEGLOVE Insights™
The trade-offs, organized around your case.
A clear, patient-facing map of the decision—built from the record, reviewed by a cardiac surgeon and cardiologist, and designed for the next conversation with your treating team.
Download a sample reportWHITEGLOVE Insights™
Your coronary decision,
organized.
Patient-facing anatomyYour vessels.
Your options.
Your priorities.
Your options.
Your priorities.
The decision already proposed
Your symptoms, testing, cath findings, medications, prior procedures, and treating team’s plan—clearly attributed to the source record.
A two-specialist perspective
A cardiac surgeon and cardiologist review the same complete record independently, then confer and co-sign one patient-facing report.
Guideline and evidence map
Professional guidance and relevant evidence placed beside the clinical details that make them applicable—or limited—in your case.
Risk, without false precision
Surgical-risk estimates and PCI-related considerations organized with model inputs, missing variables, limitations, and clinical context visible.
Your coronary anatomy
A patient-facing map connects left-main or multivessel disease, lesion location, and the important territories in your record to the decision.
CABG and PCI trade-offs
Potential benefits, burdens, durability, recovery, medication needs, and repeat-procedure considerations explained without assuming either path always wins.
What may still be missing
Incomplete imaging, testing, documentation, or unanswered questions identified for your next conversation with the treating team.
Practical next questions
A concise list grounded in the record: what to clarify, what preferences to discuss, and what information could materially change the comparison.
How it works
From scattered records to one clear next conversation.
You bring the question. WHITEGLOVEMD helps gather the evidence, convenes the Heart Team, and makes the comparison usable.
- 01
Start with a complimentary orientation
Tell a Heart Team specialist which decision you are facing. No referral or records are needed for the first conversation.
- 02
We help assemble the complete record
Upload what you have or authorize the records team to help gather cath images and reports, echocardiograms, notes, testing, labs, and recommendations.
- 03
Two specialists review independently
A cardiac surgeon and cardiologist examine the same complete record from their respective clinical perspectives, then confer.
- 04
Receive one co-signed report
Your WHITEGLOVE Insights™ report is delivered within 24 hours after the records required for the review are confirmed complete.
Clinical rigor
Source-linked reasoning, not a generic verdict.
ACC / AHA / SCAICoronary revascularization guideline hubSociety of Thoracic SurgeonsAdult cardiac surgery risk calculatorEuroSCOREEuroSCORE II risk modelAmerican Association for Thoracic SurgeryAATS risk calculator
Professional guidance, published evidence, and risk models inform—but do not replace—case-specific physician judgment. Estimates have limitations and do not predict an individual outcome with certainty.
Start with the written review
One decision.
One clear starting point.
The co-signed written review starts at $495. A live physician consultation is optional, available through higher-tier services, and costs extra.
WHITEGLOVE Insights™
$495Independent review by both physicians and one co-signed, patient-facing report.
Live physician consultation
ExtraChoose a higher-tier service only if you want live physician time in addition to the written review.
Direct-pay service. WHITEGLOVEMD does not submit insurance claims. No referral is required.
CABG versus stents FAQ
Questions patients and families ask before deciding.
Is CABG better than stents?+
There is no single answer for every patient. The comparison depends on coronary anatomy and complexity, left-main or multivessel disease, diabetes, heart function, symptoms, prior procedures, procedural risks, expected durability, medication considerations, and patient priorities. The review explains how the documented factors in your record shape the discussion without assuming one option is always superior.
What factors influence a CABG versus PCI decision?+
Important factors may include which vessels are diseased, lesion location and complexity, whether the left main or several vessels are involved, diabetes, left-ventricular function, kidney disease, bleeding or stroke risk, prior stents or surgery, completeness of revascularization, and the outcomes and burdens that matter most to you.
How do diabetes and multivessel disease affect the comparison?+
Diabetes and multivessel disease can make the longer-term evidence and the completeness of revascularization especially relevant, but they do not determine the answer by themselves. The useful comparison also considers anatomy, operative and PCI risk, heart function, other health conditions, and personal priorities.
Does left-main coronary disease always require bypass surgery?+
No single webpage or isolated finding can determine treatment. Left-main disease requires careful evaluation of lesion location and complexity, the rest of the coronary anatomy, heart function, procedural risks, and patient circumstances. Depending on the case, CABG, PCI, or further evaluation may deserve discussion with the treating Heart Team.
How are surgical risk and PCI risk compared?+
When the necessary inputs are available, the review considers three surgical-risk approaches—STS PROM, EuroSCORE II, and AATS—separately and makes missing inputs visible. PCI-related considerations may include bleeding, stroke, kidney, vascular, contrast, and antiplatelet-therapy factors documented in the record. No model predicts an individual outcome with certainty.
What are the recovery and durability differences between CABG and stents?+
PCI often involves a shorter initial recovery, while CABG generally requires a larger recovery commitment. Longer-term considerations can include completeness and durability of revascularization, graft or stent performance, the possibility of repeat procedures, and ongoing medication needs. The report puts those trade-offs in the context of your specific record.
Why do medications matter when comparing bypass with stents?+
Both strategies are usually paired with guideline-directed medical therapy. After PCI, dual antiplatelet therapy may be particularly important for a defined period, which can affect bleeding risk, adherence, and timing of other procedures. The review organizes the medications, contraindications, and practical considerations documented in your case for discussion with your treating clinicians.
Who reviews my CABG versus stents case?+
A cardiac surgeon and cardiologist independently review the same complete record, then confer and co-sign one patient-facing WHITEGLOVE Insights™ report. Their two clinical perspectives are included at every service level.
How much does a CABG versus stents second opinion cost?+
The co-signed written WHITEGLOVE Insights™ review starts at $495. A live physician consultation is optional, available in higher-tier services, and costs extra. WHITEGLOVEMD is a direct-pay service and does not submit insurance claims.
When does the 24-hour turnaround begin?+
The 24-hour turnaround begins after the records required for the review have been received and confirmed complete. Time spent requesting or collecting records is outside that window. The records team can help identify and gather what is needed with your authorization.
Do I need a referral or have to travel?+
No referral or travel is required. The medical-record review is completed remotely. You may choose the written review alone or add an optional live physician consultation through a higher-tier service.
Does WHITEGLOVEMD replace my treating doctors?+
No. WHITEGLOVEMD provides independent educational decision support and medical-record review. It does not diagnose, order, prescribe, provide emergency care, establish a treating relationship, or replace the clinicians responsible for your care.
Before you consent
Compare CABG and stents with the whole record in view.
Start with the co-signed written review. Add live physician time only if you want it.