One complete recordYour valve
decision, mapped.
decision, mapped.
01DiagnosisValve · mechanism · severity02TimingIntervene · monitor · clarify03ApproachRepair · replace · catheter
Independent heart valve second opinion
A cardiac surgeon and cardiologist review one complete record—so you can understand the diagnosis, severity, timing, and reasonable paths before your next conversation.
First, define the decision
The useful second opinion begins by separating four questions that are often compressed into one.
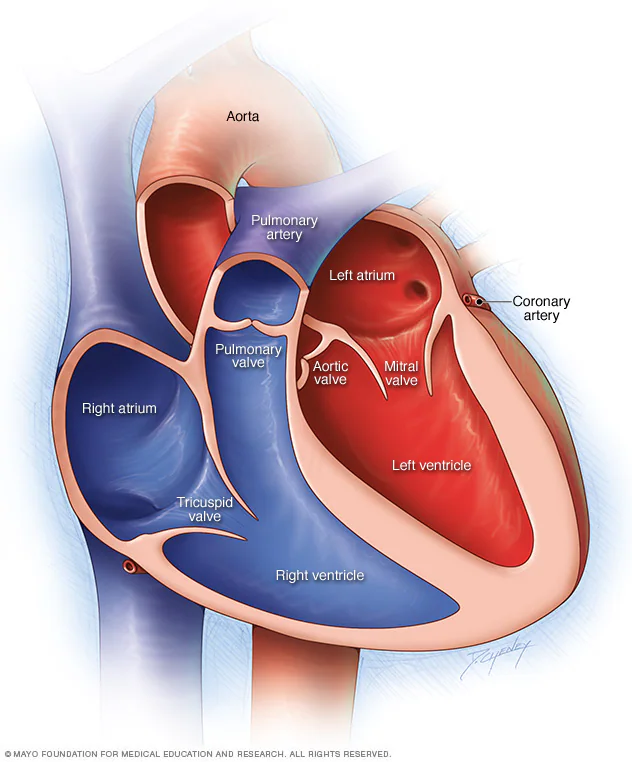
Aortic, mitral, and tricuspid disease are different decisions. The review checks the documented mechanism, severity, symptoms, heart response, and serial change before discussing timing.
Symptoms, ventricular function, chamber size, pulmonary pressure, rhythm, exercise tolerance, and progression can affect why treatment or surveillance is being discussed.
For some valve problems, repair may be relevant; for others, replacement is the expected path. Durability, anatomy, team experience, and the likelihood of a lasting result belong in the comparison.
Open, minimally invasive, and transcatheter approaches solve different problems. Anatomy, other heart disease, procedural risk, durability, and future options determine which paths are reasonable to discuss.
Three valves. Different questions.
Your report is built around the valve and mechanism documented in your own record.
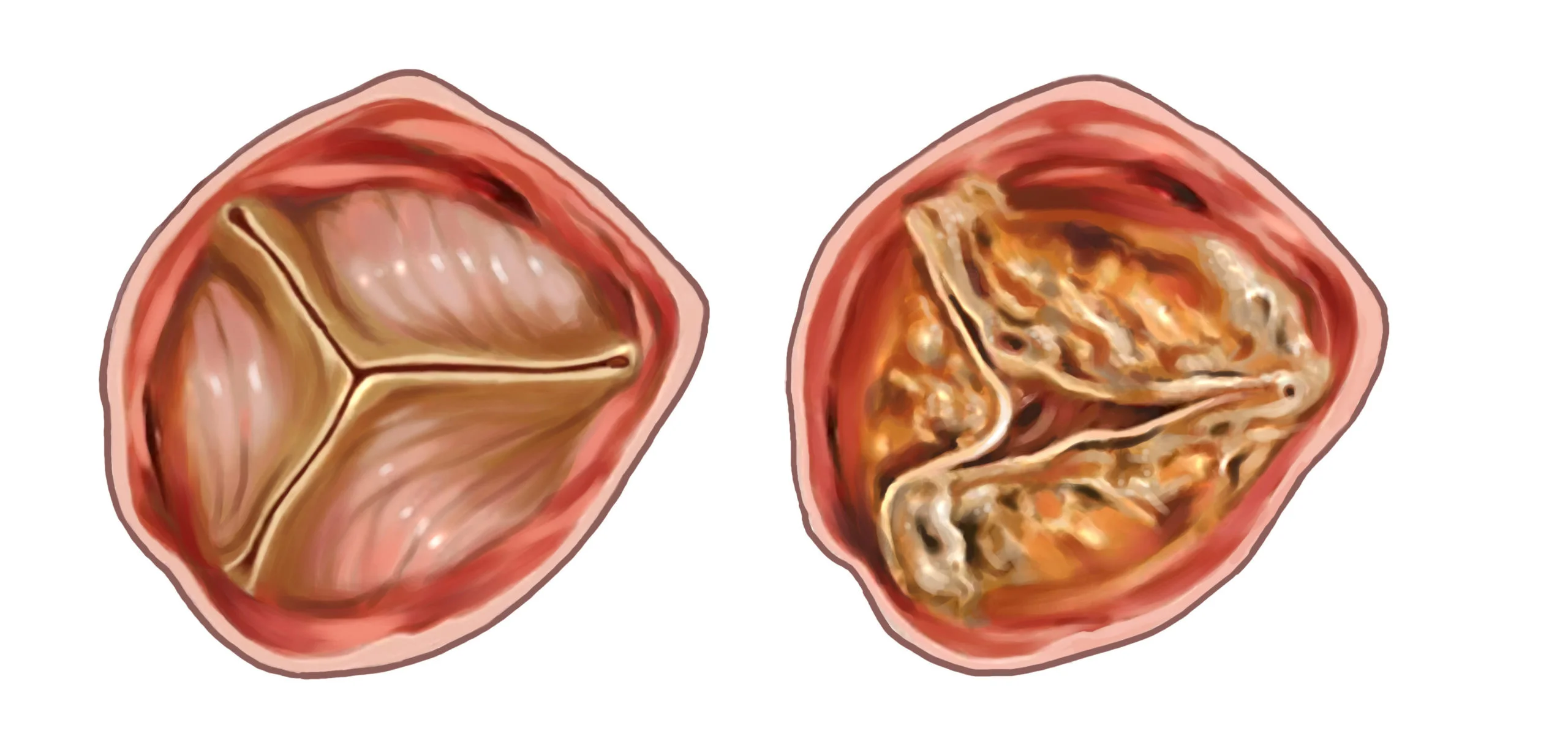
The review can organize severity, symptoms, ventricular response, aortic anatomy, TAVR versus surgery when relevant, and mechanical versus tissue prostheses if surgical replacement is being considered.
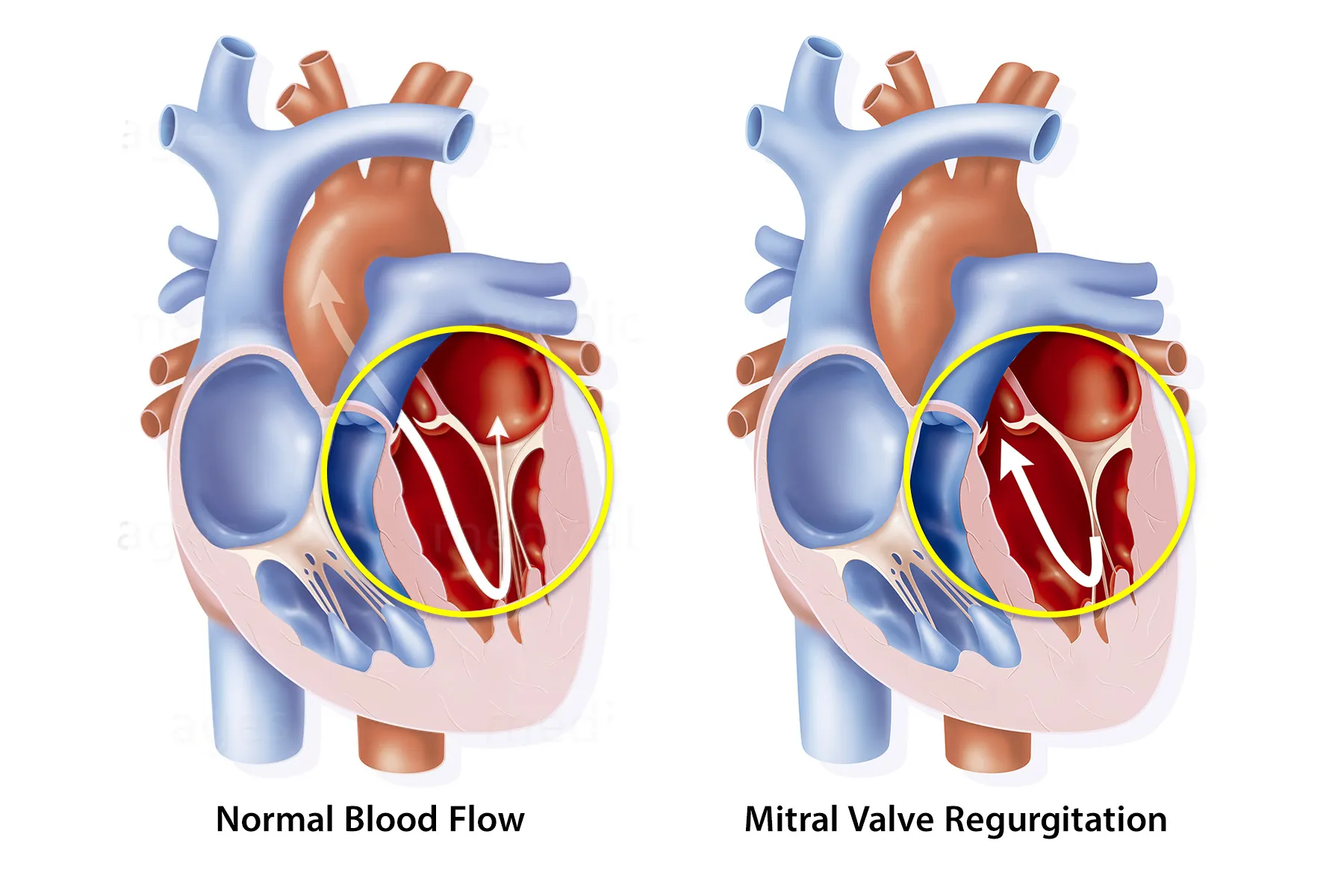
Primary and secondary mitral regurgitation are not interchangeable. The record may need to clarify mechanism, repairability, ventricular function, symptoms, surgical repair, TEER, replacement, or surveillance.
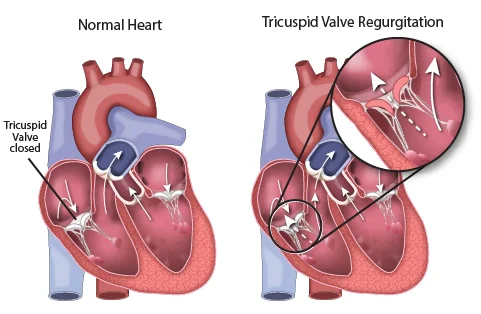
Severity, right-ventricular function, pulmonary pressure, rhythm, device leads, prior left-sided valve treatment, surgical context, and available transcatheter pathways can all matter.
Options, only when relevant
A sound review does not treat surveillance, catheter intervention, minimally invasive surgery, and open surgery as interchangeable choices. It explains why each is—or is not—part of the discussion.
Explore a sample reportWhen immediate intervention is not established, the useful question becomes what should be followed, how symptoms should be interpreted, and what findings would reopen the timing discussion.
TAVR, TEER, valve-in-valve, or another transcatheter path may be relevant for selected patients. Feasibility and trade-offs depend on the valve, anatomy, access, prior procedures, and what else needs treatment.
A smaller-incision surgical approach may be possible in selected cases. It is still heart surgery, and suitability depends on anatomy, procedure complexity, prior operations, center capability, and the need for additional procedures.
Open surgery may allow repair or replacement and can address bypass disease, an enlarged aorta, another valve, or rhythm surgery in one operation when clinically appropriate.
Beyond the first procedure
The first intervention may shape anticoagulation, durability, coronary access, reintervention, and what another procedure could require. Those trade-offs deserve one view.
 Build the plan around the person—not only the valve.
Build the plan around the person—not only the valve.If repair is being considered, the mechanism, tissue quality, expected durability, and the team’s repair experience matter more than the label alone.
When replacement is relevant, a mechanical valve generally brings greater structural durability and lifelong warfarin; a tissue valve may avoid lifelong valve-related warfarin but can deteriorate.
A future valve-in-valve or transcatheter procedure may be possible in some anatomies, but valve size, coronary access, gradients, position, and other disease can limit it.
Coronary disease, an enlarged aorta, atrial fibrillation, ventricular dysfunction, or another valve problem may change what can reasonably be accomplished in one procedure.
WHITEGLOVE Insights™
A patient-facing map of the valve question—built from the record, reviewed by both specialists, and designed for the next conversation with your treating team.
The valve, mechanism, documented severity, symptoms, heart response, serial change, and the plan already proposed—tied back to the source record.
Why intervention or surveillance is being discussed now, which documented findings carry weight, and what uncertainty remains.
When relevant, repairability, prosthesis considerations, durability, anticoagulation, and the implications of a future procedure.
Open, minimally invasive, and transcatheter paths set side by side only where the record makes them clinically relevant.
STS PROM, EuroSCORE II, and an AATS risk tool considered separately where applicable, with available inputs, missing data, and model limits visible.
Patient-facing explanations connect the echo, CT, catheterization, and operative findings to the decision—not generic education alone.
Missing imaging, measurements, testing, or clinical context that may change the conversation with the treating team.
Procedure-specific experience, public outcomes where available, repair or transcatheter capability, geography, and practical considerations when they matter.
Records, without the scavenger hunt
A valve review is only as reliable as the record underneath it. With authorization, the records team can help identify and request what is missing.
The valve mechanism and severity, ventricular response, chamber size, pulmonary pressure, and other valve findings—not only a summary line.
Anatomy, access, coronary disease, aortic dimensions, and measurements when they affect a catheter or surgical pathway.
Symptoms, examination, prior treatment, the proposed plan, and the treating clinicians’ reasoning about timing and alternatives.
Previous valve or bypass surgery, implanted valves or rings, pacemaker or defibrillator leads, and details that can change a repeat procedure.
Anticoagulation, kidney function, anemia, rhythm treatment, and other variables needed to understand risk and procedural context.
Recovery, durability, anticoagulation, future procedures, travel, caregiving, and the questions you want answered before deciding.

Your WHITEGLOVE Heart Team
A surgeon sees repairability, exposure, prosthesis strategy, combined procedures, and the consequences of reoperation. A cardiologist sees imaging, progression, rhythm, medication, catheter pathways, and long-term surveillance. Both review independently. Then they confer.
How it works
Tell a Heart Team specialist what you were told and which part of the valve decision remains unresolved. No referral or records are needed for this first conversation.
Upload what you have or authorize the records team to help identify and request the imaging, reports, notes, and proposed plan required for review.
A cardiac surgeon and cardiologist examine the same complete record from different clinical perspectives, then confer.
Your WHITEGLOVE Insights™ report is delivered within 24 hours after the records and imaging required for your review have been received and confirmed complete.
Start with the written review
Independent cardiac surgeon review. Independent cardiologist review. One physician conference. One co-signed, patient-facing report.
Frequently asked questions
Still unsure whether the review fits your situation? A complimentary orientation can help you understand the service before you proceed.
Request a free orientation callA second opinion can be useful when valve intervention has been proposed; when the diagnosis, severity, timing, or mechanism remains unclear; when you want to understand repair versus replacement, surgery versus a catheter procedure, or mechanical versus tissue valves; or when another heart problem may change the plan. It should not delay urgent or time-sensitive care directed by your treating clinicians.
The review can address aortic, mitral, and tricuspid valve disease, including stenosis, regurgitation, mixed disease, prior valve procedures, and cases involving more than one valve. The exact analysis depends on the complete medical record and the decision that is actually in front of you.
The report can organize and explain the severity documented in your records, including relevant echocardiographic measurements, symptoms, ventricular response, chamber changes, pulmonary pressure, and serial progression. It does not perform a new diagnostic examination or replace interpretation by the clinicians responsible for your care. Missing or conflicting data are identified for discussion with them.
Not for every valve or every anatomy. Repair may preserve native tissue and avoid a prosthesis in selected cases, but the likelihood and durability of a successful repair depend on the valve, mechanism, tissue, ventricular context, and team experience. Replacement may be more predictable or necessary in other cases. The report explains which questions the available record raises without choosing treatment for you.
It compares only the approaches that are relevant to the documented valve problem and anatomy. TAVR applies to selected aortic-valve cases; TEER applies to selected mitral or tricuspid cases; minimally invasive and conventional surgical approaches have different technical requirements. These are not interchangeable menu choices, and some patients need treatment of coronary disease, the aorta, another valve, or a rhythm problem at the same time.
When valve replacement is a relevant path, the report can organize the trade-offs between mechanical and tissue prostheses. These may include durability, lifelong anticoagulation, bleeding and clotting considerations, age and expected longevity, pregnancy plans when relevant, lifestyle, valve position, and possible future procedures. The final prosthesis choice belongs with you and your treating team.
Yes. The review can consider a prior repair, surgical valve, transcatheter valve, annuloplasty ring, or other cardiac procedure. Prior operative reports, implant details, current imaging, symptoms, and the new proposed plan become especially important because redo surgery, valve-in-valve treatment, another catheter procedure, and surveillance each have case-specific limits.
When applicable, the review may consider STS PROM, EuroSCORE II, and an AATS risk tool separately rather than treating them as interchangeable. Each tool has a defined population, required inputs, and limitations. The report makes available inputs and missing information visible; a risk model is one part of the decision and cannot predict an individual outcome.
The required record depends on the valve and proposed treatment. It commonly includes echocardiogram images and reports, recent clinical and procedural notes, CT imaging when relevant, catheterization or coronary assessment, prior operative reports and implant details, laboratory results, medication history, and the proposed plan. With authorization, the records team can help identify and request what is needed.
A cardiac surgeon and cardiologist independently review the same complete record, then confer and co-sign one WHITEGLOVE Insights™ report. The surgeon contributes the operative, repair, prosthesis, and technical perspective; the cardiologist contributes the imaging, longitudinal, rhythm, medication, and catheter-based perspective. Both reviews are included at every service level.
The written report is delivered within 24 hours after the records and imaging required for your review have been received and confirmed complete. Time spent identifying, requesting, transferring, or collecting records is outside that 24-hour window. Do not delay urgent or time-sensitive care while waiting for a second opinion.
The written WHITEGLOVE Insights™ review starts at $495 and includes independent review by a cardiac surgeon and cardiologist, their conference, and one co-signed report. Live physician consultation and concierge support are optional at higher service levels. The service is direct pay, and WHITEGLOVEMD does not submit an insurance claim.
The report may organize procedure-specific public outcomes, reported experience, capabilities, geography, and practical fit when those considerations are relevant and verifiable. WHITEGLOVEMD does not promise access, outcomes, affiliation, or endorsement. If you want help reaching another team, ask the care coordinator what transfer assistance may be available for your situation.
No. WHITEGLOVEMD provides independent educational decision support and medical-record review. It does not diagnose, prescribe, select a treatment, perform procedures, provide emergency care, establish a treating physician–patient relationship, or replace the clinicians responsible for your care.
Your decision stays yours
Begin with the written Heart Team review—or request a complimentary orientation if you are not sure where to start.
