One diagnosis.
Several decisions
to separate.
Your HCM pictureConnect the phenotype, symptoms, anatomy, rhythm, and options.
01FlowMeasured02RhythmReviewed03OptionsCompared
Your Incision Should Be Your Decision™
Hypertrophic cardiomyopathy second opinion
A cardiac surgeon and cardiologist independently review your complete record—then organize obstructive versus nonobstructive HCM, symptoms, medical therapy, myectomy versus alcohol septal ablation, mitral anatomy, rhythm and sudden-death questions, and specialist-center fit.
No referral or travel required. With your authorization, the records team can help obtain what is needed.
One diagnosis.
HCM is not one decision. Symptoms, obstruction, anatomy, rhythm, family context, and the proposed treatment all belong on the same page.
Explore a sample reportThe diagnosis, in context
A useful HCM review separates what is documented from what is assumed—then shows which facts support the proposed path and which questions remain unresolved.
The report separates the HCM phenotype documented in the record from the symptoms and decisions being considered. Resting, provoked, and exercise-related outflow gradients are organized rather than treated as interchangeable.
Breathlessness, chest discomfort, fainting or near-fainting, palpitations, exercise limits, and quality-of-life concerns are placed beside the rhythm, imaging, and hemodynamic findings available in the record.
Beta-blockers, nondihydropyridine calcium-channel blockers, myosin inhibitors, disopyramide, diuretics, anticoagulation, and other therapies answer different clinical questions. The report makes the documented sequence and unresolved trade-offs visible.
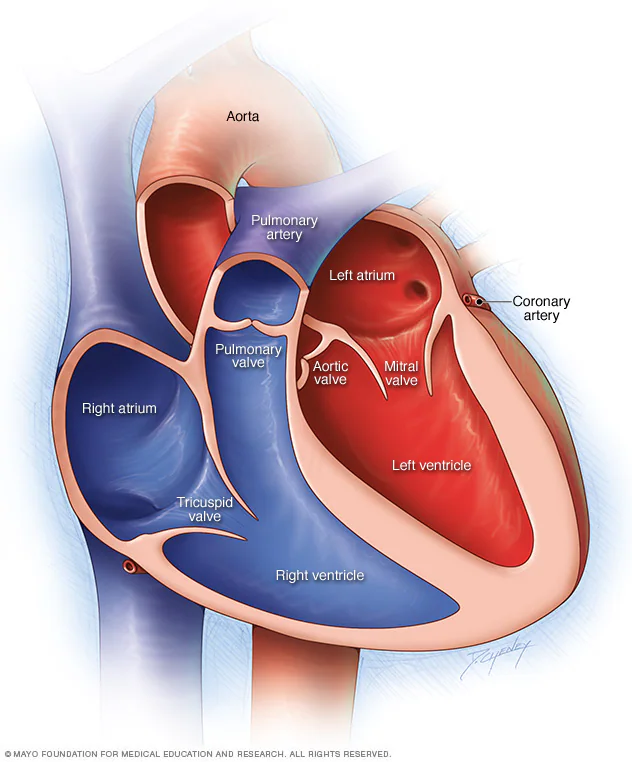
Septal thickness is only part of obstructive HCM. Systolic anterior motion, mitral regurgitation, papillary muscles, chordae, aortic-valve anatomy, and coronary disease can affect which procedural questions belong together.
Family history, prior arrest or sustained arrhythmia, unexplained syncope, wall thickness, ejection fraction, apical aneurysm, nonsustained ventricular tachycardia, and MRI scar may inform an ICD conversation.
HCM is a longitudinal disease and septal reduction is a specialized decision. Experienced multidisciplinary HCM centers, procedure-specific expertise, imaging quality, and follow-up capability deserve explicit consideration.
Septal reduction, compared
For symptomatic obstructive HCM that remains limiting despite appropriate medical treatment, septal reduction may deserve discussion at an experienced HCM center. The mechanism, anatomy, associated disease, and operator experience shape that comparison.
Myectomy directly removes part of the thickened septum and can allow surgical treatment of associated mitral, subvalvular, coronary, or other cardiac disease when those issues are present. The operation and recovery are different from a catheter-based strategy.
Alcohol septal ablation intentionally creates a controlled injury in a selected part of the septum. Suitability depends on coronary anatomy, the mechanism of obstruction, age, comorbidity, local expertise, and whether another cardiac problem requires surgery.
This service provides educational decision support. It does not diagnose HCM, prescribe medication, determine candidacy, select a procedure or device, or replace the treating clinicians.
Beyond wall thickness
HCM care can involve imaging, medical therapy, surgery, interventional cardiology, electrophysiology, genetics, exercise counseling, and longitudinal follow-up.
Resting echo alone may not answer that question. Provocative maneuvers or exercise testing can reveal clinically important outflow obstruction when it is not present at rest.
HCM, coronary disease, valve disease, rhythm disturbance, lung disease, anemia, deconditioning, and medication effects can overlap. A useful review shows what the record supports and what remains uncertain.
Mitral regurgitation may be related to systolic anterior motion, intrinsic leaflet disease, papillary-muscle anatomy, or more than one mechanism—important distinctions when a procedure is being discussed.
Cardiac MRI may clarify wall distribution, apical disease, aneurysm, ejection fraction, alternative diagnoses, and late gadolinium enhancement when those questions are relevant.
No single variable answers every sudden-death question. Major risk markers, additional modifiers, age, competing risks, device complications, and patient preferences belong in shared decision-making.
Family screening, genetic counseling, exercise, atrial fibrillation, pregnancy, heart-failure progression, and interval imaging may matter long after a single medication or procedure decision.
WHITEGLOVE Heart Team
Every service level includes both independent reviews and both physician signatures. The physicians confer before the report is finalized.
Septal, mitral, papillary-muscle, chordal, aortic-valve, and coronary anatomy; the scope of myectomy; associated procedures; and the program’s procedure-specific experience.
 WHITEGLOVE Insights™Independent reads.
WHITEGLOVE Insights™Independent reads.Symptoms, gradients, medication response, imaging, arrhythmia, device questions, genetics, family screening, functional testing, and reasonable alternatives.
WHITEGLOVE Insights™
The report is written for patients and families, but grounded in the source record, current guidance, and two physician reviews.
Download a sample report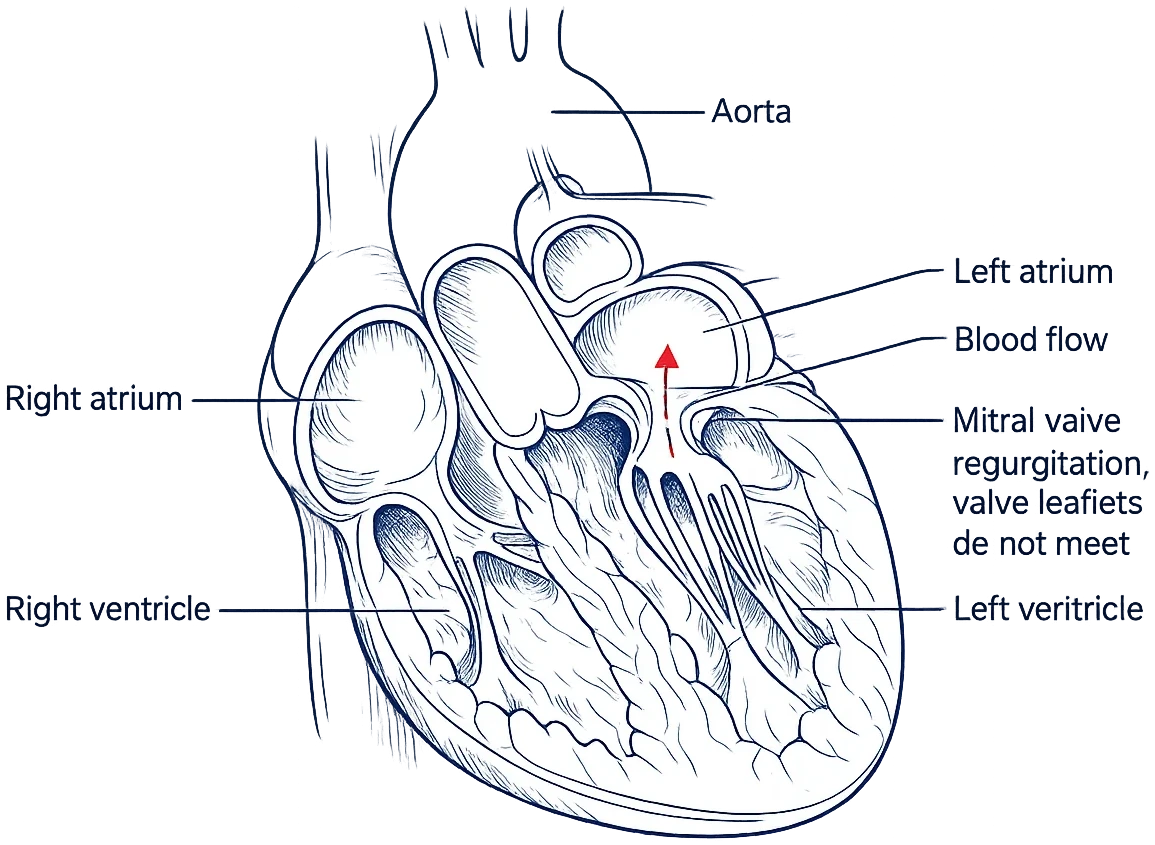
The phenotype documented in the record, symptoms, rhythm history, gradients, imaging findings, prior treatment, and the treating team’s proposed plan—clearly source-linked.
The current HCM guideline categories relevant to the documented symptoms, obstruction, medication history, imaging, arrhythmia, and procedural questions.
The reasons continued medical therapy, myosin inhibition, septal reduction, rhythm treatment, or further testing may be under discussion—with uncertainty made visible.
A patient-facing comparison of goals, anatomical requirements, burdens, limitations, and the questions that separate surgical from catheter-based septal reduction.
When relevant, the report connects systolic anterior motion, regurgitation mechanism, leaflets, papillary muscles, and chordae to the larger procedural decision.
Documented risk markers are organized for a shared ICD conversation, while model and evidence limitations remain explicit.
Unresolved gradients, absent rhythm monitoring, incomplete MRI or stress testing, family history, genetic context, and other workup gaps become useful questions.
Relevant HCM, myectomy, ablation, electrophysiology, imaging, and longitudinal-care experience is placed in front of you.
Questions raised during an optional consultation are preserved in plain language with the Heart Team’s explanation.
A concise list of records, questions, consultations, or transfer conversations to discuss with the clinicians responsible for your care.
What may still be missing
A missing study does not automatically mean care was inadequate. It means the limits of the available review should be visible—and turned into useful questions for the treating team.
The actual study and report, including septal thickness, resting and provoked gradients, systolic anterior motion, mitral regurgitation, chamber size, and ventricular function.
When symptoms and resting findings do not align, exercise echo or another appropriate provocative assessment may help clarify dynamic obstruction and functional limitation.
When relevant, MRI can add wall-thickness distribution, apical anatomy, ejection fraction, aneurysm, scar, and alternative-diagnosis context.
Electrocardiograms, ambulatory monitoring, prior atrial fibrillation or ventricular arrhythmia, syncope history, and any existing pacemaker or defibrillator data.
Which medicines were tried, at what doses, for how long, what changed, and whether side effects or other conditions limited the options.
A three-generation family history when available, prior genetic testing, counseling, and the screening plan discussed for first-degree relatives.
Evidence, with its limits visible
Guideline categories and modeled estimates describe populations and available inputs. They do not diagnose HCM, determine individual candidacy, predict an individual event, or replace clinical judgment.
How it works
The complete-record milestone matters: the 24-hour written-review clock starts only after the records and imaging required for your case have been received and confirmed.
Tell a Heart Team specialist what you were told and which part of the decision feels unresolved. No referral or records are needed for the first conversation.
Upload what you have or authorize the records team to help obtain source imaging, rhythm data, reports, clinical notes, laboratories, and the proposed plan.
A cardiac surgeon and cardiologist examine the same complete record from different clinical perspectives, then confer.
Your WHITEGLOVE Insights™ report is delivered within 24 hours after the records and imaging required for the review are complete.
Choose the support you want
Start with the written report. Add a live physician consultation or concierge access only if it fits your decision. Direct pay; no insurance claim is submitted.
Independent review by both physicians and the co-signed written report.
The written report plus a live consultation with one reviewing physician.
The written report plus both reviewing physicians together on the consultation.
The Heart Team consultation plus concierge access until the day of surgery.
Hypertrophic cardiomyopathy second opinion FAQ
A second opinion can be useful when the diagnosis or phenotype remains uncertain, symptoms and resting tests do not align, a new medication or septal reduction procedure has been proposed, myectomy and alcohol septal ablation are being compared, mitral-valve treatment is under discussion, or sudden-death risk and an ICD decision feel unresolved. It should not delay urgent or time-sensitive care directed by your treating team.
In obstructive HCM, blood leaving the left ventricle encounters a dynamic outflow obstruction, often involving the septum and systolic anterior motion of the mitral valve. In nonobstructive HCM, hypertrophy is present without that outflow gradient under the conditions tested. Symptoms and treatment questions can occur in either phenotype, and obstruction may require provocation or exercise to detect.
Yes, when that is the decision documented in the record. The report can organize prior medication trials, symptoms, gradients, anatomy, functional testing, comorbidities, and the reasons continued medical therapy, a myosin inhibitor, disopyramide, myectomy, alcohol septal ablation, or further evaluation may be under discussion. It does not prescribe a drug or select a procedure.
Myectomy is open-heart surgery that removes part of the thickened septum and can address associated mitral, subvalvular, coronary, or other cardiac disease when needed. Alcohol septal ablation is a catheter-based procedure that uses a selected septal artery to reduce tissue causing obstruction. Anatomy, age, comorbidity, associated disease, local expertise, and individual priorities affect the comparison; not every patient is a candidate for either approach.
Mitral regurgitation in HCM may result from systolic anterior motion, intrinsic leaflet disease, papillary-muscle or chordal anatomy, or more than one mechanism. The mechanism can affect whether relieving septal obstruction alone may address the leakage or whether a separate mitral strategy deserves discussion.
No. An ICD is a shared clinical decision, not an automatic result from one score or finding. The review can organize documented major risk markers and additional modifiers—including family history, syncope, wall thickness, ejection fraction, apical aneurysm, nonsustained ventricular tachycardia, and MRI scar—alongside device burdens and unanswered questions for your HCM and electrophysiology teams.
No. Current guidance uses a structured review of major risk factors and additional clinical modifiers; estimated five-year risk may add context for some patients age 16 or older. Any estimate depends on complete, accurate inputs and does not predict an individual event. Clinical judgment and shared decision-making remain essential.
Yes, when those studies are relevant and available. MRI can add anatomy and scar context, rhythm monitoring can identify atrial or ventricular arrhythmias, and exercise testing can clarify functional limitation or dynamic obstruction. The report also identifies material gaps in the available record without implying that every patient requires every test.
A cardiac surgeon and cardiologist independently review the same complete record, then confer and co-sign one WHITEGLOVE Insights™ report. Both perspectives are included at every service level. A live physician consultation is optional and costs extra.
The exact record depends on the question. It commonly includes source echocardiograms, cardiac MRI when performed, exercise or stress testing, ECGs and rhythm-monitor reports, clinical notes, medication history and response, laboratory results, family and genetic context, device records when applicable, and the proposed treatment plan. With authorization, the records team can help identify and request what is needed.
The written report is delivered within 24 hours after the records and imaging required for your review have been received and confirmed complete. Time spent requesting, transferring, or collecting records is outside that 24-hour window.
The written WHITEGLOVE Insights™ review starts at $495. A live physician consultation or concierge access can be added at higher service levels. The service is direct pay, and WHITEGLOVEMD does not submit an insurance claim.
When another specialist or center may be worth considering, the report can organize relevant HCM, myectomy, alcohol septal ablation, electrophysiology, imaging, and longitudinal-care experience, along with geography and practical fit. The team may help facilitate an introduction through its national physician and transfer network. This does not imply a formal hospital partnership or guarantee acceptance, timing, candidacy, or treatment.
Do not delay urgent or time-sensitive treatment while waiting for WHITEGLOVEMD. Fainting, severe chest pain, severe breathing difficulty, sustained rapid heartbeat, cardiac-arrest symptoms, stroke symptoms, or other possible emergencies require immediate evaluation; call 911.
The decision stays yours
Start with a complimentary orientation or begin the two-physician written review from $495.