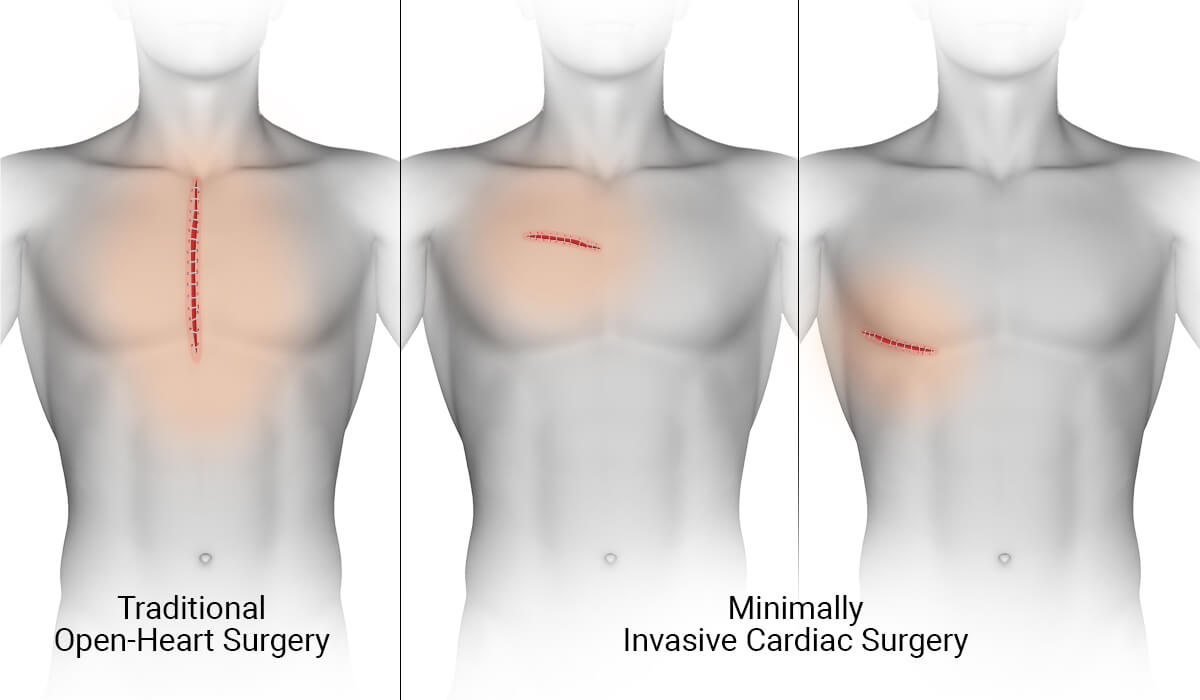
What is minimally invasive heart surgery?+
The term generally describes heart surgery performed without a full median sternotomy, but it covers very different techniques. Surgical examples include partial sternotomy, mini-thoracotomy, port-access, and robotic approaches. Catheter-based treatments are separate, non-surgical comparators. The operation being performed—not merely the incision—determines whether two paths are truly comparable.
How do I know whether I am a candidate for minimally invasive heart surgery?+
Candidacy depends on the exact procedure, valve or coronary anatomy, aorta and peripheral vessels, chest anatomy, prior surgery or radiation, other disease that may need treatment, overall risk, and the experience of the proposed team. A complete-record review can organize those factors, but the treating physicians make the procedural decision.
Is minimally invasive heart surgery safer than open-heart surgery?+
Not automatically. A smaller incision may offer recovery or comfort advantages in selected patients, but safety also depends on exposure, completeness of treatment, procedure and bypass time, vascular access, conversion planning, the patient’s risk factors, and the team’s experience. The most appropriate access is case-specific.
Is robotic heart surgery the same as minimally invasive surgery?+
Robotic surgery is one minimally invasive technique. The surgeon controls the instruments from a console while the operation is performed through ports and a small working incision. Other minimally invasive operations do not use a robot, and many catheter-based procedures are performed by a different route entirely.
Can aortic-valve replacement be performed through a smaller incision?+
Selected surgical aortic-valve replacements can be performed through a partial sternotomy or right thoracotomy. TAVR is a separate catheter-based option. The reasonable comparison depends on age, anatomy, surgical risk, coronary access, durability, other required surgery, and lifetime valve strategy.
Can mitral-valve repair be performed robotically or through a mini-thoracotomy?+
Selected mitral repairs can be performed through a right mini-thoracotomy or with robotic assistance at experienced centers. Whether that route is reasonable depends on repair complexity, valve and coronary findings, vascular access, prior operations, other procedures that may be needed, and the program’s results with that exact approach.
Can bypass surgery be minimally invasive?+
Some patients may be considered for minimally invasive direct coronary bypass, robot-assisted coronary surgery, or a hybrid approach combining bypass and catheter treatment. Coronary target location, number of vessels, conduit plan, completeness of revascularization, emergency access, and program experience are central to the comparison.
Can AFib surgery or a Maze procedure be minimally invasive?+
Selected surgical ablation procedures may be performed through limited incisions, thoracoscopically, or in hybrid programs. The relevant choice depends on AFib history, atrial anatomy, valve disease, stroke-prevention needs, prior ablation, and whether another heart operation is planned.
Does a smaller incision always mean a faster recovery?+
No. Incision size can influence pain and mobility, but the operation itself, bypass time, lung function, complications, rehabilitation, frailty, and support at home also affect recovery. Claims about recovery should be tied to the exact procedure and patient, not the label alone.
What if a minimally invasive procedure must be converted to open surgery?+
Conversion is sometimes the safest response to limited exposure, bleeding, unexpected anatomy, or another intraoperative problem. A useful preoperative conversation should include the team’s reasons for conversion, its experience managing it, and whether immediate full access is available.
Who reviews my case, and what do I receive?+
A cardiac surgeon and cardiologist independently review the same complete record, confer, and co-sign one WHITEGLOVE Insights™ report. The written review begins at $495. A live physician consultation is optional and costs extra.
How quickly is the written report delivered?+
The written report is delivered within 24 hours after the records and imaging required for the review have been received and confirmed complete. Time spent requesting or transferring records is outside that 24-hour window.
Does insurance cover the review?+
WHITEGLOVEMD is a direct-pay educational decision-support and independent medical-record review service. The written Heart Team review starts at $495, and WHITEGLOVEMD does not submit an insurance claim. Live consultation is optional and costs extra.
Does WHITEGLOVEMD recommend a specific operation or replace my treating surgeon?+
No. WHITEGLOVEMD provides educational decision support and independent medical-record review. It does not diagnose, prescribe, select a procedure, or replace the treating physicians. The report helps patients and families ask better questions and discuss reasonable options with the clinicians responsible for their care.