01Medical therapy
Treat the disease without a procedure
Medication, cardiac rehabilitation, risk-factor treatment, and symptom management may be the main strategy or part of every strategy.
Before you choose an approach
Your Incision Should Be Your Decision™
Some patients have a reasonable non-open option. Others do not—and should not delay the operation they need. A cardiac surgeon and cardiologist review your complete record to compare medical therapy, catheter-based procedures, minimally invasive surgery, surveillance, and full open surgery in the context of your anatomy and goals.
No referral or travel required. Live physician consultation is optional and costs extra.

Your record may support
The short answer
Sometimes. But “can it be avoided?” is different from “should it be avoided?” The right alternative must treat the same clinical problem with a reasonable balance of completeness, safety, durability, recovery, and future options.
A diagnosis name alone cannot answer the question. The decision depends on disease severity, imaging, procedural anatomy, symptoms, urgency, other conditions that need treatment, and your priorities.
Five possible pathways
These paths can overlap. Medication may continue before and after a procedure; surveillance may lead to intervention later; and a minimally invasive operation is still an operation.
Medication, cardiac rehabilitation, risk-factor treatment, and symptom management may be the main strategy or part of every strategy.
Examples include PCI with stents, TAVR, mitral TEER, selected valve-in-valve procedures, catheter ablation, and some endovascular aortic repairs.
Selected valve, coronary, and rhythm operations may use a partial sternotomy, mini-thoracotomy, thoracoscopic, robotic, or hybrid approach.
When intervention criteria are not yet met, scheduled clinical follow-up and repeat imaging may be the appropriate plan.
A sternotomy-based operation may remain the most complete, durable, or technically appropriate path, especially when several problems must be addressed together.
Diagnosis by diagnosis
These are decision frameworks, not treatment recommendations. Only the treating team can determine procedural eligibility after clinical evaluation.
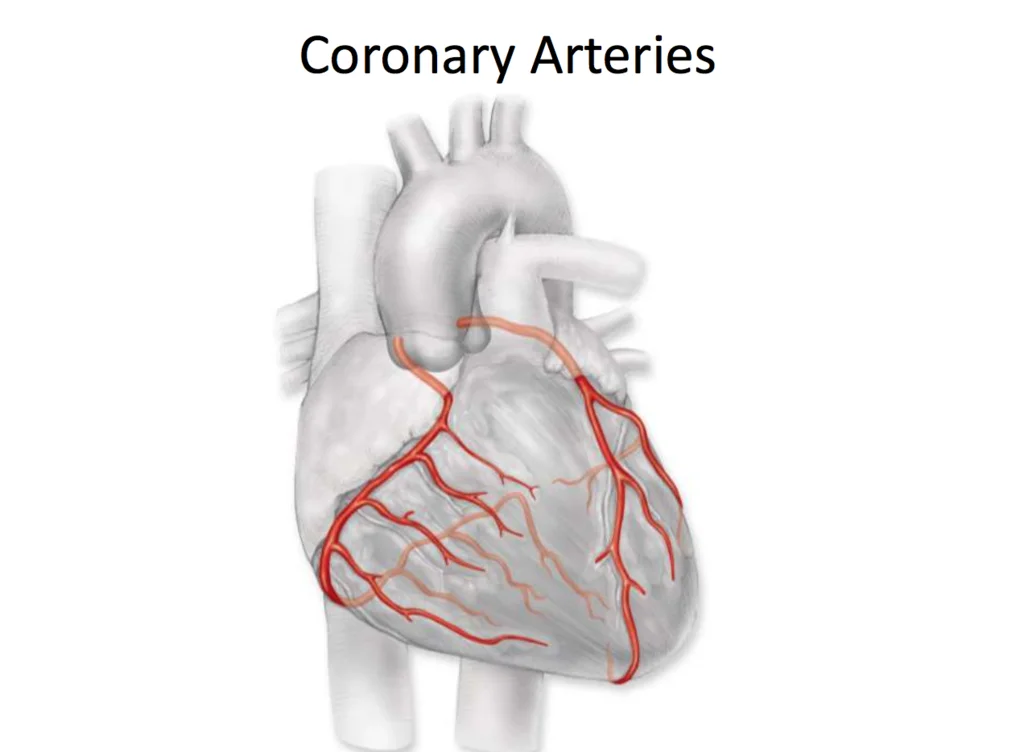
Guideline-directed medical therapy is foundational. PCI with stents may be reasonable for selected coronary patterns, clinical settings, and patient priorities.
CABG may remain favored when coronary disease is more complex, complete revascularization is unlikely with PCI, or other clinical factors change the balance.
Coronary angiogram and images, vessel locations, disease complexity, symptoms, ischemia, heart function, diabetes status, prior treatment, and the proposed graft or stent plan.
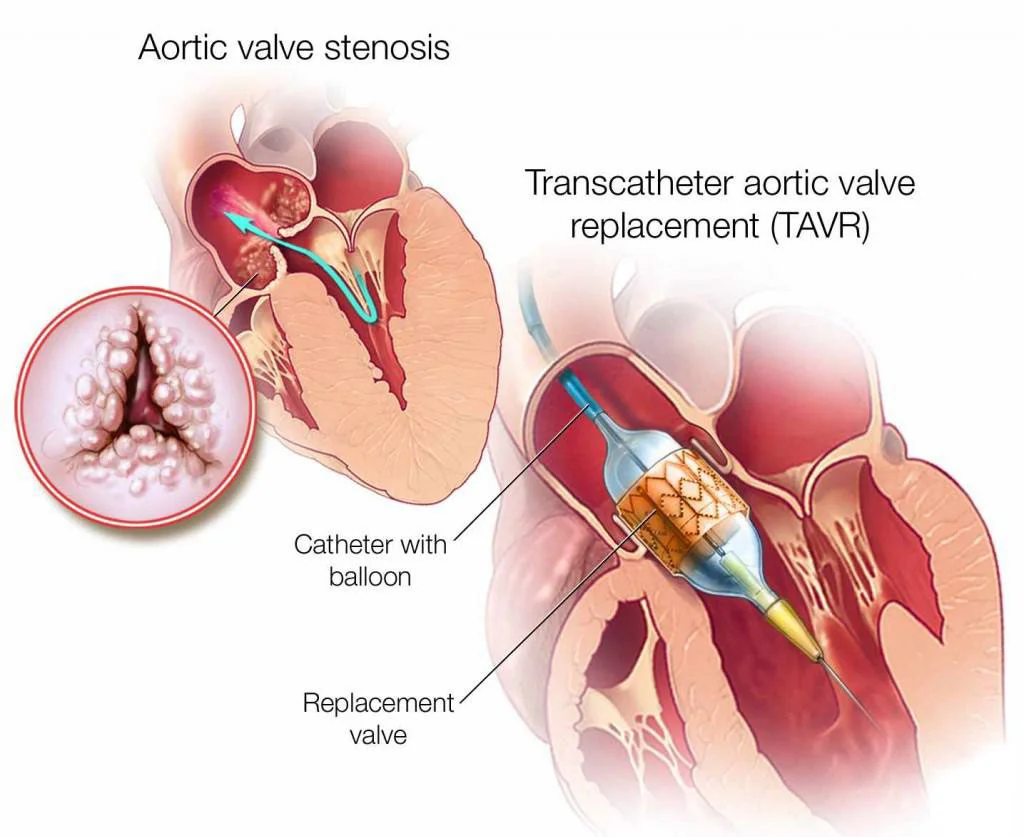
For selected severe aortic stenosis, TAVR may be an alternative to surgical valve replacement. Earlier disease may be monitored. The comparison is different for aortic regurgitation.
SAVR may better fit some patients because of valve anatomy, lifetime valve strategy, coronary access, durability considerations, or another operation that is needed at the same time.
Echocardiogram images and measurements, CT sizing when available, valve morphology, coronary anatomy, symptoms, exercise findings, age and life expectancy, surgical risk, and other valve or aortic disease.
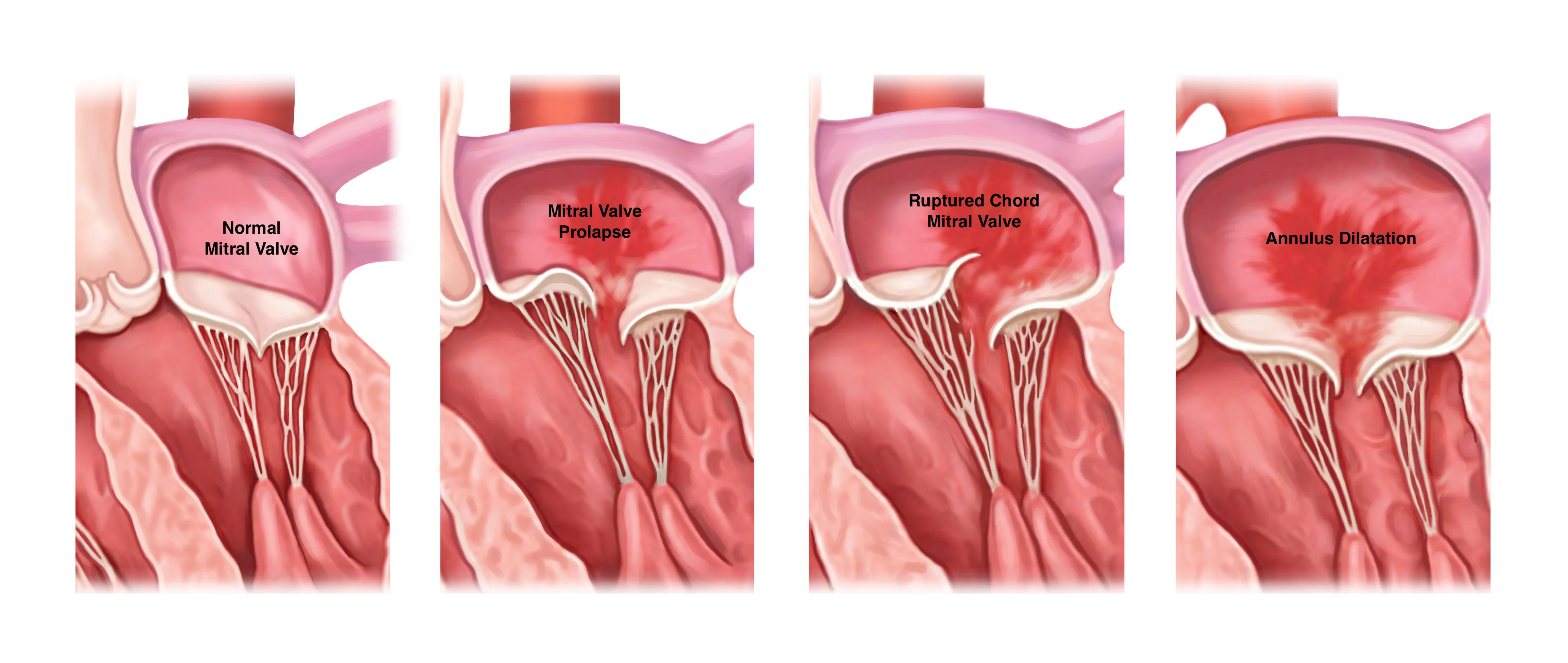
Medication can address symptoms and related heart failure. Selected patients may be considered for transcatheter edge-to-edge repair or another catheter-based therapy.
Surgical repair or replacement may offer a more complete or durable treatment for some valve anatomy, particularly when a durable repair is likely or other cardiac work is required.
Transthoracic and transesophageal echo images, mechanism and severity of regurgitation or stenosis, ventricular size and function, pulmonary pressures, symptoms, rhythm history, coronary findings, and repair feasibility.
Rate or rhythm medications, cardioversion, catheter ablation, and selected left atrial appendage occlusion strategies may be considered depending on symptoms and stroke or bleeding risk.
A surgical ablation or Maze procedure is often considered in the context of another planned heart operation, although selected stand-alone or hybrid approaches exist.
AFib type and duration, symptom burden, monitoring, atrial size, heart function, prior cardioversion or ablation, medication response, stroke risk, bleeding history, and any valve disease.
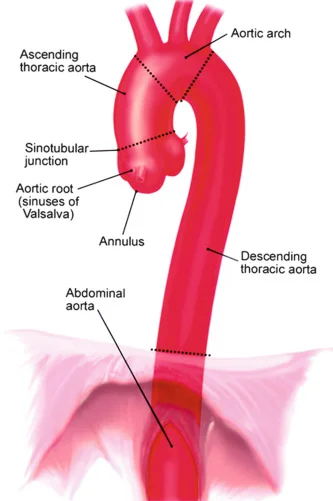
Blood-pressure management and serial imaging may fit stable disease below an intervention threshold. TEVAR may fit selected descending thoracic aortic anatomy.
Aortic root, ascending aorta, and arch disease often has a different technical pathway, and open repair may remain necessary when anatomy or urgency requires direct reconstruction.
CT or MRI images, aortic segment and measurements, growth over time, symptoms, valve anatomy, genetic or family history, body size, access vessels, and whether the condition is stable or acute.
What changes the answer
A useful comparison makes the inputs explicit. It should also identify what cannot yet be concluded because a report, image, measurement, or risk input is missing.
“Heart disease” is not one decision. Coronary, valve, rhythm, and aortic conditions have different treatment thresholds and alternatives.
Measurements, symptoms, progression, heart function, and the expected course without intervention help determine whether treatment is needed now.
Valve shape, coronary pattern, aortic segment, access vessels, prior operations, chest anatomy, and imaging quality can expand or narrow the options.
A catheter procedure may address one problem. Open surgery may sometimes address coronary, valve, rhythm, and aortic disease in one operation.
The comparison should include procedural risk, the risk of deferring treatment, recovery, repeat intervention, and the limits of any risk estimate.
Age, life expectancy, future coronary access, future valve options, and the likelihood of another procedure can matter beyond the next recovery.
The proposed approach should be evaluated in the context of the team’s procedure-specific experience, conversion plan, and available backup.
Recovery priorities, caregiving, travel, work, tolerance for repeat procedures, and personal preferences belong in shared decision-making.

The decision behind the incision
Recovery matters. So do completeness, durability, the chance of another intervention, and what happens if treatment is deferred. The best decision is the one that holds those tradeoffs together.
Ask whether your case fitsWHITEGLOVE Heart Team
A cardiac surgeon evaluates operative indication, access, completeness, repair, and technical alternatives. A cardiologist evaluates diagnostic context, medical therapy, imaging, catheter options, and longitudinal care.

Reviews whether an operation is indicated, which surgical access or repair may fit, what open surgery can accomplish, and what a less-invasive path may leave untreated.
Reviews the diagnosis, medical therapy, disease trajectory, imaging, catheter-based possibilities, and whether surveillance or further testing may be reasonable.
WHITEGLOVE Insights™
The report is educational decision support—not a remote treatment order. It organizes the evidence, tradeoffs, and next questions around your documented case.
See a sample reportDecision focus
What the record says is being treated, how severe it appears, and why a decision is being considered now.
The imaging and procedural features that may support or limit medication, catheter, minimally invasive, surveillance, or open paths.
Where the documented facts map to relevant clinical guidance—along with any facts that remain missing or uncertain.
Validated estimates when applicable, the inputs used, material limitations, and risks of both intervention and deferral.
A case-specific comparison of potential benefits, tradeoffs, unknowns, and why an option may not fit.
A practical list to take back to the cardiologist, surgeon, structural heart team, or aortic team responsible for your care.
Published clinical framework
These specialty sources describe how decisions are structured. They do not determine which treatment is appropriate for any individual patient.
ACC/AHA/SCAI guidance recommends a multidisciplinary Heart Team when the optimal coronary revascularization strategy is unclear and emphasizes shared decision-making.
American College of Cardiology · 2021 coronary revascularization guidelineValve guidance and a 2026 joint specialty-society statement emphasize multidisciplinary evaluation, anatomy, long-term outcomes, and an individualized lifetime strategy.
ACC, SCAI & STS · Aortic valve replacement decision-making statementCurrent AFib guidance describes roles for medical therapy, catheter ablation, and selected percutaneous left atrial appendage occlusion based on symptoms and individualized risk.
American College of Cardiology · 2023 atrial fibrillation guidelineAortic disease guidance covers medical therapy, imaging surveillance, endovascular repair, open surgery, and shared decision-making across distinct aortic conditions.
American College of Cardiology · 2022 aortic disease guidelineHow it works
One coordinated process, completed remotely, with records support available.
Choose the $495 written review or request a complimentary orientation call. No referral or travel is required.
Upload what you have or authorize help gathering the notes, reports, original imaging, and proposed treatment plan needed for the review.
A cardiac surgeon and cardiologist examine the same complete record from different clinical perspectives, then confer.
The 24-hour turnaround begins only after all records and imaging required for your review have been received and confirmed complete.
Begin in writing
The written review does not require a live appointment. Optional consultation choices are available for patients who want to discuss the report with a reviewing physician.
Independent review by a cardiac surgeon and cardiologist, their conference around the decision, and one co-signed written report.
Add a live conversation if you want to discuss the written review with one or both reviewing physicians.
Frequently asked questions
Depending on the diagnosis and anatomy, the reasonable paths may include guideline-directed medical therapy, a catheter-based procedure, a minimally invasive surgical approach, structured surveillance, or full open surgery. These are not interchangeable. The right comparison depends on what is being treated, how severe it is, what the imaging shows, what else needs treatment, procedural risk, expected durability, and the patient’s goals.
No. Some people can reasonably use a non-open path, while others need open surgery for the most complete, durable, or urgent treatment. An alternative is only useful when it can address the actual disease and anatomy without creating an unacceptable tradeoff. A review should explain both when an alternative fits and when it does not.
Sometimes medical therapy is the primary treatment, and it is foundational in many cardiac conditions. But medication cannot mechanically open every blocked artery, replace a severely diseased valve, repair every aneurysm, or reverse every structural problem. Whether it can defer or replace a procedure depends on the diagnosis, severity, symptoms, heart function, and expected risk without intervention.
PCI with stents can be an alternative to CABG for selected coronary anatomy and clinical situations. The comparison depends on which vessels are involved, disease complexity, diabetes, heart function, symptoms, feasibility of complete revascularization, bleeding considerations, prior treatment, and patient goals. Some coronary patterns still favor bypass surgery.
TAVR can be an alternative to surgical aortic-valve replacement for many patients with severe aortic stenosis, but not for everyone. Valve anatomy, access vessels, age and life expectancy, surgical risk, coronary access, durability, bicuspid anatomy, aortic disease, and the need for another cardiac procedure can change the choice. Aortic regurgitation is a different decision and may have fewer catheter-based options.
Transcatheter edge-to-edge repair, often called TEER, may be an option for selected mitral regurgitation when the valve anatomy and clinical context fit. Surgical repair or replacement may still offer a more complete or durable result for other patients. The mechanism of regurgitation, ventricular function, symptoms, pulmonary pressures, repairability, surgical risk, and other needed procedures all matter.
No. Minimally invasive heart surgery is still surgery. It may use a partial sternotomy, small thoracotomy, ports, robotic assistance, or a hybrid approach, and it may still require cardiopulmonary bypass. Catheter-based treatment is a separate category. A smaller incision should be weighed against completeness, safety, conversion planning, and the team’s experience.
Structured surveillance may be appropriate when disease has not reached an intervention threshold, symptoms are absent or stable, heart function remains acceptable, measurements are below a treatment threshold, or the balance of risk does not yet favor a procedure. The treating team should define the follow-up interval, repeat imaging, symptom triggers, and findings that would change the plan.
Depending on the AFib pattern and the treatment goal, options may include rate-control or rhythm-control medication, cardioversion, catheter ablation, anticoagulation for stroke prevention, or selected left atrial appendage occlusion. These address different parts of AFib care. A surgical Maze is often considered when another heart operation is already planned, but stand-alone and hybrid pathways may be considered in selected cases.
Some stable aortic disease can be managed with blood-pressure treatment and scheduled imaging. Selected descending thoracic aneurysms may be treated with endovascular repair when anatomy is suitable. Aortic root, ascending aorta, and arch disease often follows a different pathway and may require open reconstruction. Sudden chest or back pain, fainting, stroke symptoms, or rapid deterioration may signal an emergency and requires immediate emergency care.
Open surgery may remain the best fit when direct access is needed, several cardiac problems should be treated together, anatomy is unfavorable for a catheter approach, a durable repair is more likely surgically, endovascular access is inadequate, or the condition is urgent. Choosing open surgery after comparing alternatives is not a failure; it may be the most appropriate plan.
The $495 WHITEGLOVE Insights™ review includes independent medical-record review by a cardiac surgeon and cardiologist, their conference around the decision, and one co-signed patient-facing written report. It is designed to organize the documented diagnosis, anatomy, options, tradeoffs, uncertainties, and questions to discuss with the treating team.
Yes. A live physician consultation is optional and available at an additional cost. You can begin with the $495 written dual-physician review and decide whether a live conversation would be useful after reviewing the available service options.
The 24-hour turnaround begins only after all medical records and original imaging required for the review have been received and confirmed complete. Time spent requesting, transferring, or clarifying missing materials is outside the 24-hour review window.
No. WHITEGLOVEMD provides educational decision support and independent medical-record review. It does not diagnose, prescribe, order treatment, choose a procedure, provide postoperative care, or replace the clinicians responsible for your care. Use the report to support a shared conversation with your treating team.
Do not wait for an online review. Call 911 or seek immediate emergency care for new or severe chest pain, severe shortness of breath, fainting, stroke symptoms, sudden severe chest or back pain, or rapid worsening. WHITEGLOVEMD is not an emergency service, and a records review should never delay urgent evaluation or treatment.
Do not delay urgent care
Call 911 or seek immediate emergency care for new or severe chest pain, severe shortness of breath, fainting, stroke symptoms, sudden severe chest or back pain, or rapid worsening. Ask the treating team whether there is time for another review in any urgent situation.
Before the approach is final
Begin with the $495 written dual-physician review, or request a complimentary orientation call if you want help deciding whether the service fits.
