One complete-record review
Root. Valve.
Ascending aorta.
- 01
- Measure the anatomy
- 02
- Compare the valve paths
- 03
- Review the complete operation
Your Incision Should Be Your Decision™
Aortic root surgery second opinion
A cardiac surgeon and cardiologist independently review your complete record—then organize root and ascending-aorta measurements, valve-sparing versus composite-graft context, bicuspid or connective-tissue considerations, additional cardiac procedures, risk, and center experience.
The written review is $495. A live physician consultation is optional and costs extra. No referral or travel is required.

One complete-record review
A root operation is more than a diameter: anatomy, valve durability, the complete procedure, and the team performing it all belong in one review.
See a sample reportThe decision, in context
The report does not choose an operation. It makes the documented reasoning, trade-offs, and open questions visible so you can discuss them with the treating team.
The root, sinotubular junction, tubular ascending aorta, and arch are distinct parts of one connected problem. The report organizes which segments are enlarged and exactly what the proposed operation would replace.
CT, MRI, and echocardiography can measure the aorta differently. Source images, measurement technique, body-size context, and reliable serial comparison help explain why timing is being discussed.
Valve-sparing context depends on cusp tissue, valve geometry, stenosis or regurgitation, the mechanism of leakage, and whether a durable repair appears technically plausible—not age alone.
A bicuspid valve, Marfan syndrome, Loeys–Dietz syndrome, another heritable aortopathy, or a family history of aneurysm or dissection can change the questions around timing, procedure scope, and surveillance.
Coronary disease, a separate valve problem, arch involvement, prior cardiac surgery, or a need for bypass can change the operation’s complexity and whether an isolated root procedure tells the whole story.
Valve-sparing root replacement and complex root or arch operations are experience-sensitive. Procedure-specific experience, a multidisciplinary aortic program, and public outcomes when available belong in the discussion.
Two root-replacement contexts
These are not interchangeable labels, and neither is automatically right for everyone. The relevant comparison depends on the actual valve, aortic anatomy, lifetime implications, and procedure-specific experience.
The diseased root is replaced while the patient’s own aortic valve is retained and supported within or alongside the graft. The operation may avoid a prosthetic valve, but suitability and durability depend on valve tissue, geometry, repair needs, anatomy, and operator experience.
A composite graft operation—often called a Bentall procedure—replaces the aortic root and valve with a valved conduit, then reconnects the coronary arteries. If this path is being considered, mechanical-versus-tissue valve trade-offs become part of the lifetime plan.
The procedure names above are educational context, not a recommendation or a determination of candidacy.
Map the operative scope
A useful second opinion connects each measurement and finding to the part of the operation it may affect.
Valve annulus, sinuses, coronary origins, and the transition into the ascending aorta. Root replacement involves the coronary attachments and may preserve or replace the valve.
The tubular segment above the root may be enlarged with or without major root involvement. An ascending-only graft does not answer every valve or root question.
Some plans extend from the root into the ascending aorta or arch and may add valve, coronary-bypass, or other cardiac work. Each added component changes the risk and experience conversation.

WHITEGLOVE Heart Team
The cardiac surgeon examines operative scope, valve preservation or replacement, coronary reimplantation, additional procedures, technical risk, and center fit. The cardiologist places that plan beside serial imaging, valve function, coronary disease, medical context, and the longitudinal strategy.
WHITEGLOVE Insights™
Patient-facing does not mean generic. The analysis stays tied to source imaging, the complete record, current guidance, and the limits of what is known.
Explore a sample report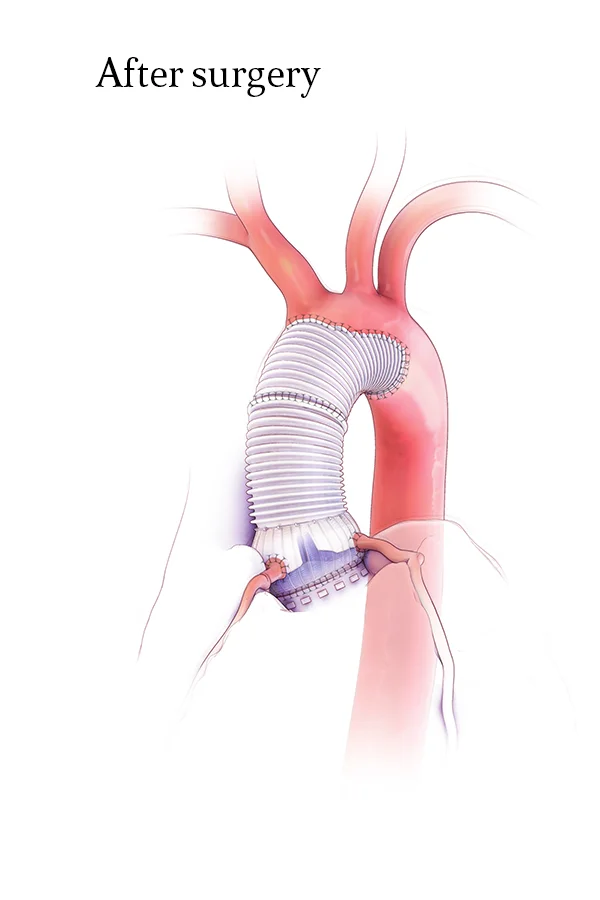
Root, ascending-aorta, and arch measurements are organized by study and date, with non-comparable measurements and imaging limitations made visible.
The documented size, change over time, body-size context, symptoms in the record, valve findings, family history, and treating team’s reasoning are placed together.
The report explains the available valve morphology, function, cusp quality, leakage mechanism, repair questions, and factors that may affect durability.
The reasons a Bentall or another valved-conduit strategy may be under discussion, plus prosthesis and future-management questions, are explained in patient-facing language.
Concomitant valve, coronary-bypass, ascending-aorta, arch, rhythm, or redo components are connected to the overall plan instead of reviewed in isolation.
The STS ascending-aorta and aortic-root model and other applicable tools are interpreted alongside anatomy, health history, planned procedures, and model limitations.
Procedure-specific experience, multidisciplinary capability, public outcomes when available, geography, and practical considerations are organized for discussion.
Missing records, unresolved findings, and concise questions are gathered for the next conversation with the physicians responsible for your care.
Complete-record review
A missing study does not decide the case. It should make the limits of the review visible and become a specific question for the treating team.
The actual images and reports showing the root, ascending aorta, arch, and coronary origins—not only a measurement copied into a clinic note.
Earlier CT, MRI, or echocardiogram studies needed to judge whether apparent growth is real and whether the measurement technique is comparable.
Valve morphology and function, stenosis or regurgitation, ventricular response, and other valve findings relevant to preservation or replacement.
Catheterization, CT coronary information, or other testing when coronary disease or coronary anatomy could change the operative plan.
History, medications, laboratory results, prior operations, functional status, family history, genetic testing, and connective-tissue diagnosis when relevant.
The surgeon’s notes, consent language, planned graft and valve strategy, other procedures, and the proposed hospital or aortic program.
Evidence, interpreted
Measurements, genetic context, valve findings, planned procedures, and clinical judgment determine how population guidance relates to one person.
How it works
The complete-record milestone is explicit: the 24-hour written-review window begins only after every record and image required for the case is received and confirmed complete.
Choose the $495 written review when you are ready, or request a complimentary orientation call first. No referral is required.
Upload what you have. With your authorization, the records team can help identify and request the source imaging, reports, notes, testing, and proposed plan needed for review.
A cardiac surgeon and cardiologist examine the same complete record from their respective perspectives, then confer on the final analysis.
Your WHITEGLOVE Insights™ report is delivered within 24 hours only after the records and imaging required for your review have been received and confirmed complete.
Start with the written review
The written review stands on its own. Add live physician time only if you want it.
Aortic root surgery FAQ
Clear answers begin with the complete anatomy, valve findings, proposed operation, and your clinical context.
Discuss your caseAortic root surgery treats the part of the aorta attached to the heart, where the aortic valve and coronary arteries connect. Depending on the anatomy and valve, an operation may preserve the native valve, replace the root and valve together with a composite graft, and/or extend into the ascending aorta or arch. The exact scope should be clear before consent.
A second opinion can be useful when root surgery has been proposed, measurements are close to a decision threshold, studies disagree, valve-sparing and composite-graft approaches are both being discussed, or bicuspid valve disease, connective-tissue disease, coronary disease, arch involvement, or prior heart surgery makes the plan more complex. It should not delay urgent or time-sensitive care directed by your treating team.
No. The root and tubular ascending aorta are adjacent but distinct segments. Enlargement may involve one or both, and a proposed operation may extend across the root, ascending aorta, or arch. Source imaging and segment-specific measurements are needed to understand the actual anatomy and operative scope.
Valve-sparing root replacement replaces the diseased root while retaining the patient’s native aortic valve, sometimes with additional valve repair. A Bentall procedure replaces the root and valve together with a valved conduit and reconnects the coronary arteries. Each approach has anatomy, durability, prosthesis, follow-up, and experience considerations. The review explains those factors without selecting a procedure for you.
Sometimes, but not for every valve or every patient. The discussion can depend on cusp tissue quality, bicuspid or tricuspid morphology, stenosis, the mechanism and severity of regurgitation, root geometry, whether cusp repair is needed, expected durability, and the surgeon’s valve-sparing experience. The treating surgical team determines technical candidacy.
Either may be considered, depending on the clinical situation. A mechanical valve is designed for long durability but generally requires lifelong anticoagulation. A tissue valve may avoid lifelong warfarin but can deteriorate and create future reintervention questions. Age, bleeding and clotting context, pregnancy considerations when relevant, lifestyle, and future options belong in shared decision-making.
A bicuspid valve can be associated with enlargement of the root or ascending aorta and may have stenosis, regurgitation, or cusp anatomy that affects preservation or replacement questions. A useful review considers the valve and the entire proximal aorta together rather than treating the diameter as the only issue.
Yes, when relevant and documented. A specific genetic diagnosis, syndromic features, age, body size, family history of aneurysm or dissection, pregnancy considerations, and prior genetic evaluation can change the guideline context, operative questions, and surveillance discussion for the patient and relatives.
Yes. Coronary disease, another valve problem, arch involvement, rhythm surgery, and prior cardiac operations can change the scope and risk of a root operation. The report organizes the complete proposed procedure so a root decision is not evaluated as if it were happening alone.
Root operations are technically complex, and different programs may have different experience with valve-sparing, composite-graft, arch, genetic-aortopathy, and redo cases. The review can organize procedure-specific experience, multidisciplinary aortic capability, and public outcomes when available. It does not guarantee a particular outcome or imply a hospital partnership.
The exact record depends on the case. It commonly includes source CT or MRI images and reports, serial imaging, echocardiogram images and reports, clinical and surgical notes, coronary assessment when relevant, laboratory results, medication and medical history, genetic or family context, and the proposed operative plan. The records team can help identify what is required.
A cardiac surgeon and cardiologist independently review the same complete record, then confer and co-sign one WHITEGLOVE Insights™ report. The operating-room and longitudinal cardiology perspectives are included in the written review.
The WHITEGLOVE Insights™ written review is $495. A live physician consultation is optional, is not required to receive the written report, and costs extra. WHITEGLOVEMD is a direct-pay service and does not submit an insurance claim.
The written report is delivered within 24 hours only after the records and imaging required for your review have been received and confirmed complete. Time spent identifying, requesting, transferring, or collecting missing records is outside the review window.
No. WHITEGLOVEMD provides educational decision support and independent medical-record review. It does not diagnose, prescribe, select a procedure, perform surgery, establish a treating physician–patient relationship, provide emergency care, or replace the clinicians responsible for your care. The decision remains with you and your treating team.
Do not delay urgent or time-sensitive treatment while waiting for WHITEGLOVEMD. Sudden severe chest or back pain, fainting, stroke symptoms, severe shortness of breath, or another possible emergency requires immediate evaluation; call 911.
The decision stays yours
Start the $495 written review, or request a complimentary orientation call if you are not sure what records you need.
