Does the diagnosis support an operation?
The symptoms, imaging, testing, and documented severity should be considered together—not reduced to one finding.
Before you consent
Your Incision Should Be Your Decision™
The honest answer cannot come from a diagnosis alone. A cardiac surgeon and cardiologist review your complete record, evaluate why surgery is being proposed, and organize the indication, timing, alternatives, and risk into one co-signed report.
No referral or travel required. We can help collect your records.
The short answer
Surgery may be the clearest path. Another approach may deserve discussion. A test or risk input may still be missing. A useful review does not promise agreement or disagreement; it makes the reasoning visible before a consequential decision.
If your situation may be emergent, seek immediate medical care. An online records review is not emergency care and should never delay it.
What “necessary” really means
The decision is not simply surgery versus no surgery. It is whether the recommendation, timing, approach, and setting fit your specific record.
The symptoms, imaging, testing, and documented severity should be considered together—not reduced to one finding.
Timing can depend on symptoms, progression, anatomy, heart function, and what may happen if treatment is deferred.
When relevant, the review compares surgery with catheter-based, minimally invasive, medical, or monitoring pathways.
Procedure-specific experience, public outcomes, clinical complexity, geography, and transfer options can all matter.
When another review helps
None of these proves that the recommendation is wrong. Each is a reasonable signal that the decision deserves a more complete review.
You know an operation was recommended, but not which findings make it necessary or why the timing matters.
You have heard about surgery, stents, TAVR, TEER, medication, monitoring, or a minimally invasive option—but not how they compare for you.
Multiple valves, redo surgery, aortic work, multivessel disease, frailty, or major comorbidities can make the tradeoffs less straightforward.
New imaging, new symptoms, or another clinician’s opinion altered the plan and you want the reasoning reconciled.
You want to know what supports operating now, what could reasonably wait, and what should be monitored if surgery is deferred.
A confirming review can be valuable when it explains why the current plan fits and what alternatives were considered.
The complete record
The review should connect what you feel, what the tests show, what is proposed, and what remains uncertain.
Consultation notes, symptoms, diagnoses, prior procedures, medications, and relevant medical history.
Echocardiograms, catheterization reports and images, CT or MRI studies, laboratory results, and rhythm testing when relevant.
The operation, timing, planned approach, hospital, and any alternatives already discussed.
Missing studies, conflicting measurements, incomplete risk inputs, or questions the record does not yet answer.
WHITEGLOVE Heart Team
A cardiac surgeon evaluates the operative questions. A cardiologist evaluates the diagnostic, medical, and non-operative context. They review independently, confer, and co-sign the report you receive.
Indication, anatomy, operative approach, technical alternatives, perioperative considerations, and procedure fit.
Diagnostic context, medical therapy, catheter-based alternatives, imaging, and longitudinal cardiac perspective.
WHITEGLOVE Insights™
Every page turns a part of the record into something you can use with your treating team.
Download a sample report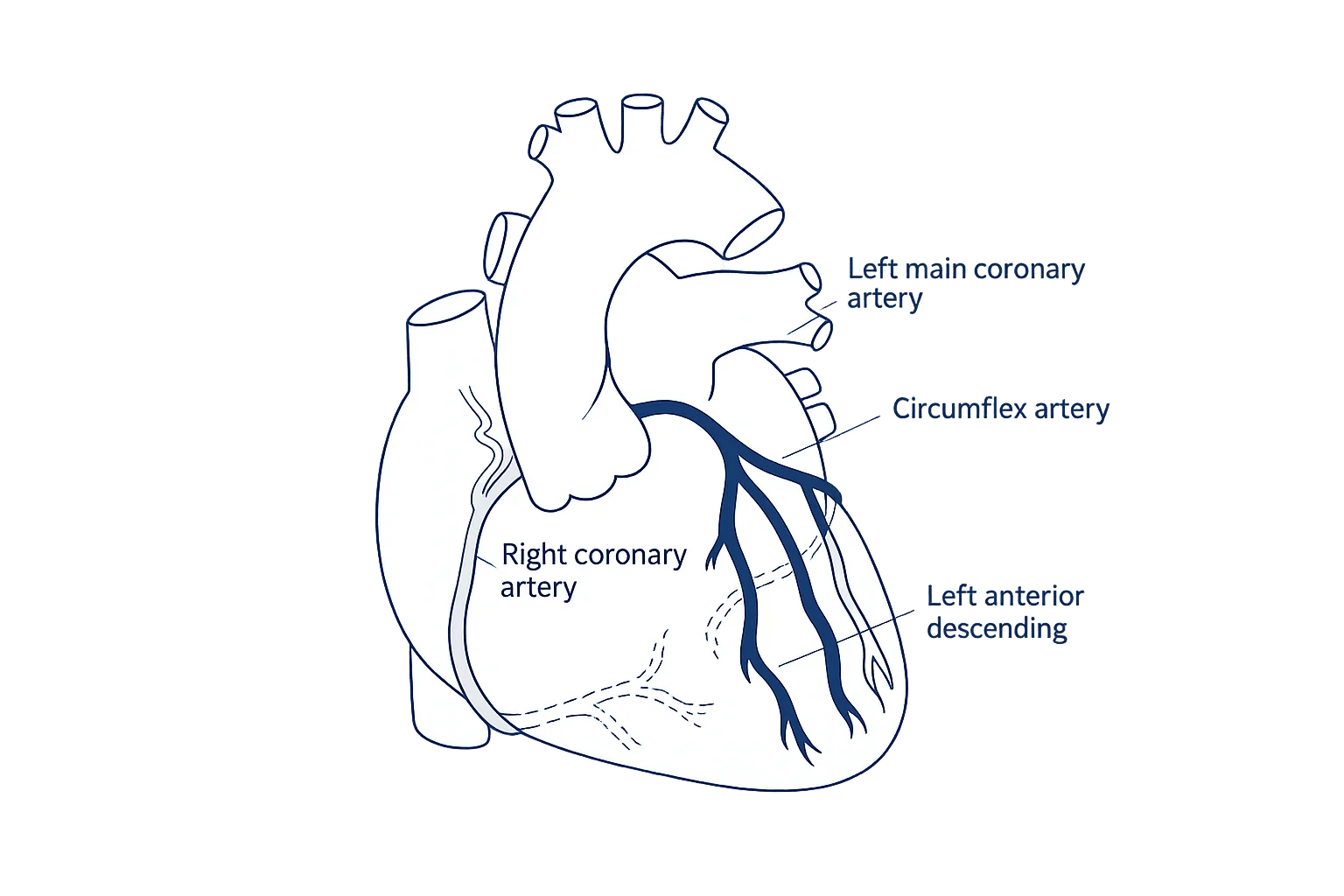
The diagnosis, symptoms, testing, and proposed plan—clearly tied to the source record.
Where the documented decision sits within current guidance and which facts make it relevant.
Validated models considered with their inputs, missing variables, and limitations made visible.
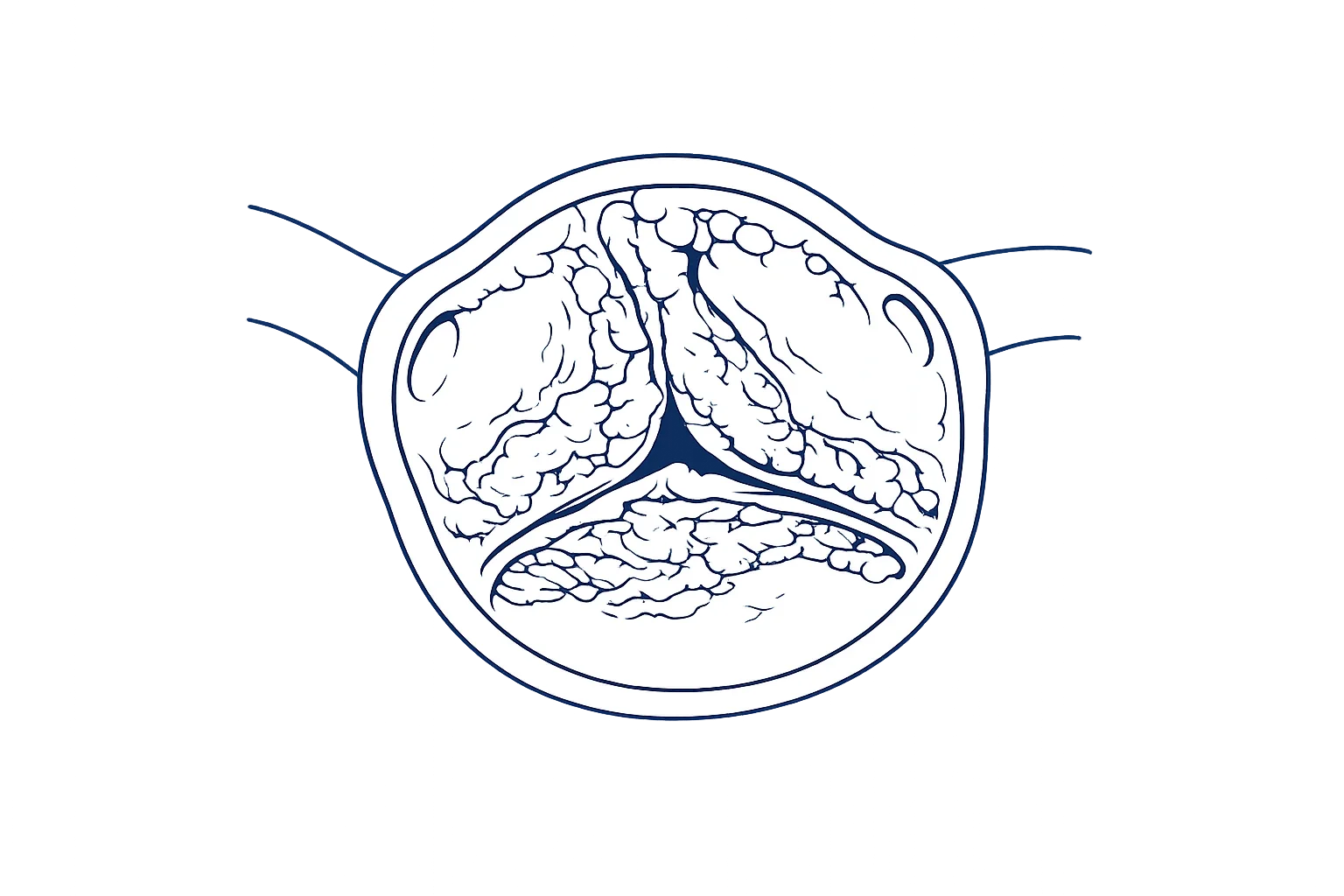
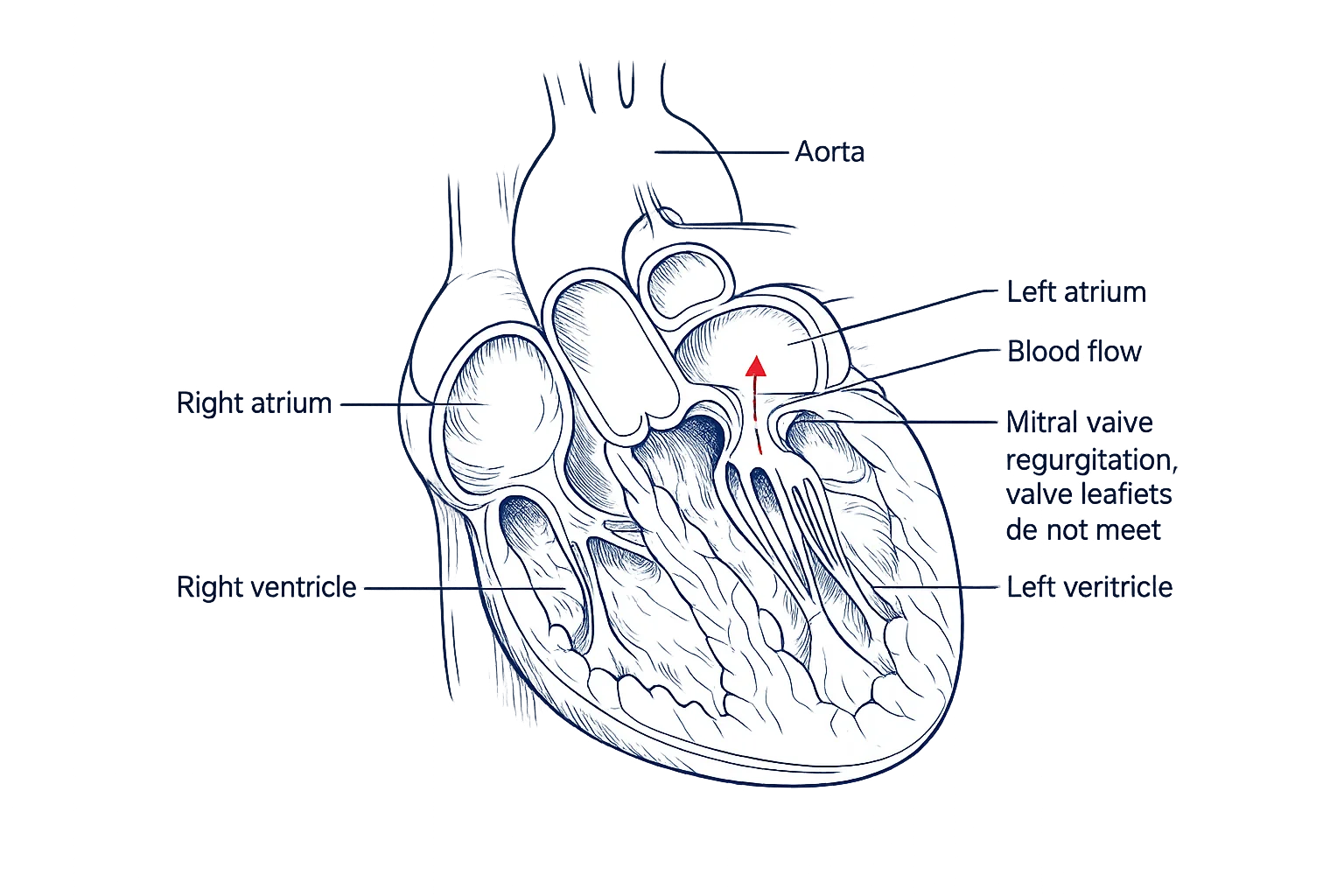
Patient-facing visuals and explanations linked to the findings in your own record.
Surgical, catheter-based, minimally invasive, medical, or monitoring paths compared when relevant.
What may still be missing and what to discuss with your treating cardiologist and surgeon next.
Published clinical framework
These sources describe how clinical decisions should be structured. They do not determine whether surgery is necessary for any individual person.
The 2021 ACC/AHA/SCAI coronary revascularization guideline emphasizes a multidisciplinary Heart Team, patient preferences, and shared decision-making when the optimal strategy is unclear.
American College of Cardiology · 2021 guideline key perspectivesACC/AHA valve guidance describes shared decision-making that considers the lifetime risks and benefits of valve type and transcatheter versus surgical approaches.
American College of Cardiology · Valvular guideline implementationThe Society of Thoracic Surgeons describes its operative risk calculator as a tool for estimating procedure-specific mortality, major morbidity, and short-term outcomes from current national data.
Society of Thoracic Surgeons · ACSD Operative Risk CalculatorHow it works
One coordinated process—without asking you to chase every record alone.
Choose a review or request a complimentary orientation call. No referral or records are needed for that first conversation.
Upload what you have or authorize our records team to help collect reports, imaging, notes, and the proposed plan.
A cardiac surgeon and cardiologist examine the same complete record, then confer around the decision.
The 24-hour turnaround begins after the complete records needed for review have been received and confirmed.
Choose your level of physician time
Every tier includes independent review by a cardiac surgeon and cardiologist and a co-signed written report.
The written, co-signed Heart Team review.
The report plus a live consultation with one reviewing physician.
The report plus both reviewing physicians together on the consultation.
The Heart Team consultation plus concierge access until the day of surgery.
FAQ
No diagnosis or website can answer that by itself. A useful review considers the complete record: symptoms, imaging, test results, disease severity, heart function, relevant medical history, the proposed operation, timing, and reasonable alternatives. WHITEGLOVEMD has a cardiac surgeon and cardiologist review those materials independently and bring both perspectives together in one co-signed report.
Another review can be especially useful before you consent, when the explanation is unclear, more than one approach may fit, the case is complex or high-risk, recommendations conflict, new test results changed the plan, or you want to understand why surgery is being recommended now.
Yes. A valuable review does not need to disagree with the original recommendation. Confirmation can help by making the indication, timing, alternatives, risk, and unanswered questions easier to understand before you move forward.
When those alternatives are relevant to the documented anatomy and clinical situation, the report can compare open surgery with catheter-based, minimally invasive, medical, or monitoring pathways. It also explains when an alternative may not fit the record.
Every WHITEGLOVEMD case is reviewed independently by a cardiac surgeon and a cardiologist. They then confer and co-sign one patient-facing WHITEGLOVE Insights™ report.
The exact record depends on the decision, but it may include cardiology and cardiac-surgery notes, echocardiograms, catheterization reports and images, CT or MRI studies, laboratory results, medication lists, prior procedure records, and the proposed operative plan. With your authorization, our records team can help gather and organize them.
The 24-hour turnaround begins after the complete records needed for the review have been received and confirmed. Time spent obtaining missing records is outside that 24-hour window.
WHITEGLOVE Insights™ is $495, WHITEGLOVE Consult is $995, WHITEGLOVE Heart Team is $1,495, and WHITEGLOVE Concierge is $2,495. Every tier includes independent review by a cardiac surgeon and cardiologist and a co-signed written report.
No referral is required, and the medical-record review is completed virtually. You can begin from home, and our records team can help obtain the clinical information needed for the review.
Use the documented reasoning and questions to continue the conversation with your treating clinicians. WHITEGLOVEMD provides independent educational decision support; it does not direct treatment or replace the clinicians responsible for your care.
No. WHITEGLOVEMD provides educational decision support and independent medical-record review. It does not diagnose, order, prescribe, treat, manage emergencies, provide postoperative care, or replace your treating clinicians.
Do not wait for an online second opinion. Call 911 or seek immediate emergency care for possible emergency symptoms such as new or severe chest pain, severe shortness of breath, fainting, stroke symptoms, or rapid worsening. Ask your treating team whether there is enough time for another review in any urgent situation.
Before the first incision
Start with the written Heart Team review—or request a complimentary call if you want to talk it through first.