What is a TAVR second opinion?+
A TAVR second opinion is an independent review of the aortic-valve diagnosis, imaging, proposed transcatheter procedure, surgical alternative, risk context, and unanswered questions. At WHITEGLOVEMD, a cardiac surgeon and cardiologist review the complete record independently and co-sign one patient-facing WHITEGLOVE Insights™ report.
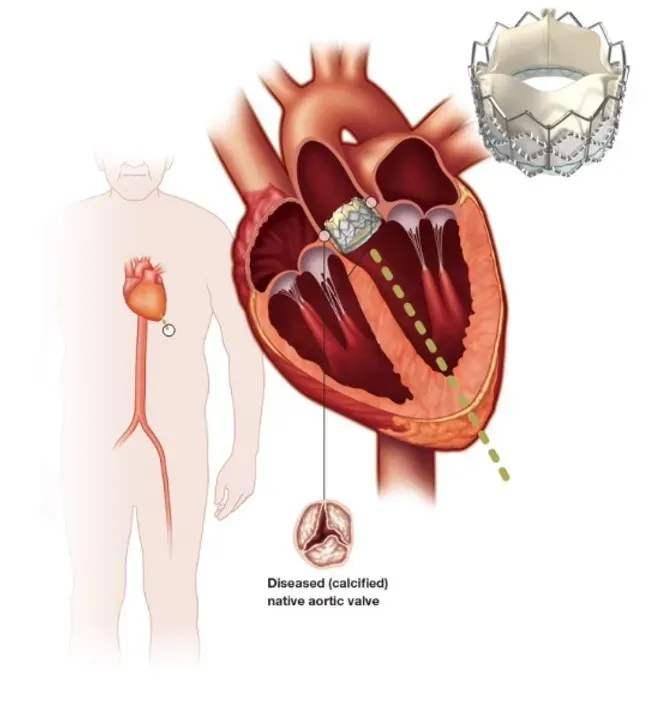
Is TAVR the same as open-heart surgery?+
No. TAVR places a replacement aortic valve through a catheter and does not require the same open surgical approach as surgical aortic valve replacement. The procedures have different access requirements, technical capabilities, recovery profiles, limitations, and future implications. The treating Heart Valve Team determines whether either approach is appropriate.
How do doctors compare TAVR with surgical valve replacement?+
The comparison can include symptoms, valve severity, age and anticipated longevity, surgical risk, frailty, transfemoral access, valve and aortic anatomy, coronary disease, other valves, prior operations, expected durability, coronary access, future valve options, and patient goals. No single factor determines the answer in every case.
Does age alone decide between TAVR and surgery?+
No. Age and anticipated longevity are important, but they are not the only considerations. Anatomy, access, other cardiac disease, surgical risk, valve durability, future coronary and valve procedures, functional status, and patient preferences also matter. A treating Heart Valve Team must individualize the choice.
Can someone be too low-risk for TAVR?+
Predicted surgical risk is only one part of the decision. Current U.S. valve guidance considers age, expected longevity, transfemoral feasibility, anatomy, indications for intervention, and shared decision-making in addition to surgical risk. Device labeling, local expertise, and the treating team’s evaluation also apply.
What imaging is usually important for a TAVR review?+
The exact record varies, but it may include echocardiography, the TAVR planning CT with source images, cardiac catheterization or coronary imaging, ECG, laboratory results, specialist notes, and prior operative or valve records. Upload what you have; the records team can help identify and request missing materials with authorization.
Why do coronary arteries and the aorta matter?+
Coronary height and access, the aortic annulus and root, calcification, bicuspid anatomy, ascending-aortic disease, and coronary artery disease can influence procedural feasibility, complications, whether another problem needs treatment, and the options available later. These details require review of the actual record and imaging.
Can TAVR treat a bicuspid aortic valve?+
TAVR may be considered in selected patients with bicuspid anatomy, but suitability is case-specific. Valve shape and calcification, aortic-root and ascending-aortic dimensions, coronary anatomy, access, age, expected longevity, and the need for other surgery all require careful evaluation by the treating Heart Valve Team.
What if I also have blocked coronary arteries or another valve problem?+
Additional coronary, valve, rhythm, or aortic disease can change the comparison because surgery may allow more than one problem to be addressed in a single operation, while staged or catheter-based strategies may be possible in selected cases. The report organizes the documented options and tradeoffs for discussion with your treating team.
Does the review calculate my risk?+
When applicable and supported by complete inputs, the review considers validated procedure-specific risk models and explains their limitations. A calculator does not capture every anatomical, functional, frailty, or technical factor and cannot predict an individual outcome with certainty.
How much does the written TAVR review cost?+
WHITEGLOVE Insights™ starts at $495. It includes independent review by a cardiac surgeon and cardiologist, their conference around the decision, and one co-signed written report. Higher tiers add optional live consultation and concierge support.
When does the 24-hour turnaround begin?+
The 24-hour medical-review window begins only after all records and imaging required for the case have been received and confirmed complete. Time spent requesting or obtaining missing materials is outside that window.
Do I need a referral or need to travel?+
No referral is required, and the medical-record review is completed virtually. Travel is not required for the review. An in-person evaluation may still be required by any team considering a procedure.
Will WHITEGLOVEMD tell me which procedure to choose?+
WHITEGLOVEMD provides educational decision support and independent medical-record review. The report organizes the evidence, reasonable pathways, tradeoffs, uncertainties, and questions. It does not diagnose, prescribe, determine candidacy, choose a procedure, or replace the clinicians responsible for your care.
What symptoms mean I should seek emergency care now?+
Call 911 or seek immediate emergency care for new or severe chest pain, severe shortness of breath, fainting, stroke symptoms, or rapid worsening. Do not wait for an online records review when symptoms may represent an emergency.