Your Incision Should Be Your Decision™
CABG second opinion
Before bypass surgery, see the whole coronary decision.
A cardiac surgeon and cardiologist independently review the documented coronary anatomy, symptoms, heart function, testing, proposed bypass plan, and alternatives that may be relevant—then confer and co-sign one patient-facing report.
What happens next: A member of our team will call within 2 business hours. During business hours, a same-day conversation with a cardiac surgeon or cardiologist may be arranged only when clinically appropriate and a physician is available.
- 2
- independent physician reviews
- 1
- co-signed written report
- 24 hr
- only after all required records and imaging are received and confirmed complete
No referral or travel required. With your authorization, the records team can help obtain what is needed. $495 includes the two-physician written review and co-signed report. Live physician consultation begins with WHITEGLOVE Consult at $995.
Case mapCoronary anatomy
WHITEGLOVE Heart TeamSurgeon + cardiologist
The question is not only “bypass or stents?” It is “which path fits this anatomy, this risk, and this life?”
Message Us about my decisionThe decision in front of you
Four questions a CABG review should make clearer.
There is no generic answer to bypass versus stents. The useful answer is grounded in your anatomy, symptoms, testing, health, goals, and the guideline-directed care that remains foundational with either path.
Does the record support bypass surgery?
The review brings the coronary anatomy, symptoms, ischemia testing, heart function, and proposed targets into one clinical picture.
Do other paths deserve comparison?
When relevant, CABG is considered beside PCI or stenting, guideline-directed medical therapy alone, or further evaluation—without implying that every option fits every patient.
What would the operation need to accomplish?
The report examines the proposed targets, completeness of revascularization, and conduit considerations documented in your case.
What risk and setting fit this case?
Procedure-appropriate risk estimates, missing inputs, comorbidities, procedure-specific experience, and public center outcomes are placed in context.
Built from the reviewed record set
What shapes a coronary revascularization decision.
The report does not reduce the decision to one blockage or one risk score. It organizes the details that can change how the options are understood.
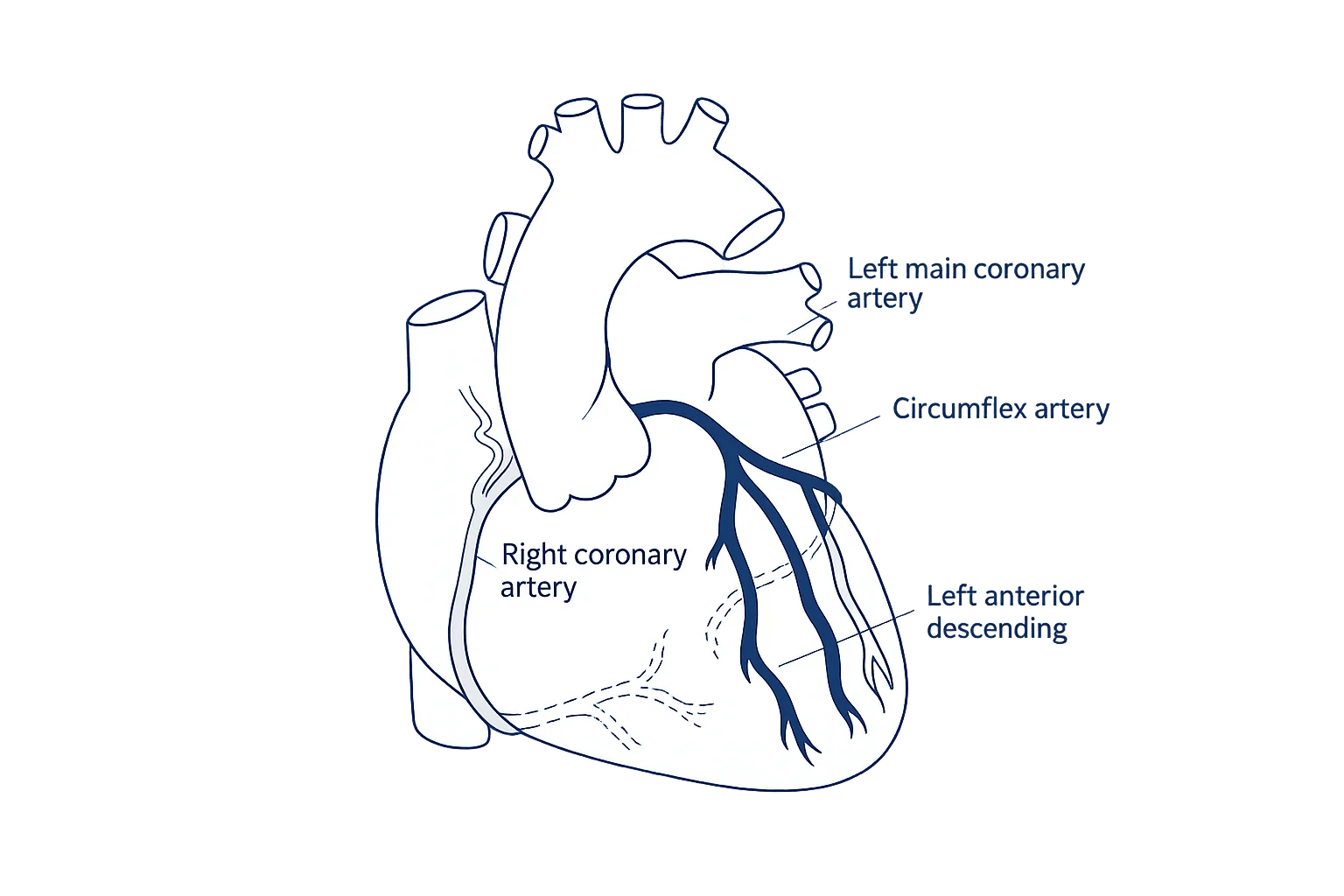
Coronary anatomy
Which vessels are narrowed, where the disease sits, whether left main or multivessel disease is present, and how complex the pattern appears.
Symptoms and ischemia
The symptoms, functional limits, prior testing, and documented evidence that heart muscle is not receiving enough blood.
Diabetes and other conditions
Diabetes, kidney or lung disease, prior stroke, frailty, and other factors that may affect both strategy and operative risk.
Left-ventricular function
Ejection fraction, regional wall motion, valve findings, and whether additional testing or viability context may matter.
Revascularization plan
The proposed bypass targets, whether the documented plan addresses the important territories, and where uncertainty remains.
Conduit considerations
Internal mammary and radial-artery considerations, vein grafts, and the case-specific reasons a conduit strategy may or may not fit.
Options, in context
Not “which treatment is best?”
Which path fits this record?
CABG and PCI are procedural paths. Guideline-directed medical therapy and risk-factor management remain foundational with either and may be the primary strategy in some cases. The review makes that context—and any need for more information—visible.
CABG
Surgical revascularization considered in the context of anatomy, symptoms, heart function, diabetes, operative risk, targets, and the proposed plan.
PCI or stenting
A catheter-based path considered when relevant to anatomy, complexity, prior treatment, procedural risk, and the goals of care.
Guideline-directed therapy
Lifestyle measures, medications, and risk-factor management remain foundational. The review distinguishes when this may be the primary strategy and what generally continues alongside CABG or PCI; medication changes remain with the treating clinicians.
More information first
When the record leaves important uncertainty, the report identifies the imaging, testing, documentation, or clinical question that may help resolve it.
WHITEGLOVE Insights™
Every page should add something you can use.
A patient-facing map of the CABG decision—built from the record, reviewed by a cardiac surgeon and cardiologist, and designed for the next conversation with your treating team.
Download a sample reportWHITEGLOVE Insights™
Your bypass decision,
organized.
Patient-facing anatomyYour vessels.
Your findings.
Your decision.
Your findings.
Your decision.
The plan already proposed
Your diagnosis, symptoms, cath findings, testing, medications, and treating team’s plan—clearly attributed to the source record.
CABG, PCI, and medical context
Reasonable paths compared when they are clinically relevant, including why a path may or may not fit the documented anatomy and circumstances.
Guideline and evidence map
The decision placed beside current professional guidance and the patient-specific details that make the guidance relevant.
Individual surgical risk
The current STS ACSD operative-risk estimate is considered when applicable, with its inputs, missing variables, date, and limitations made visible. Other scores are discussed only when documented in the source record.
Your coronary anatomy
A patient-facing map connects the important vessels and lesions in your record to the decision in front of you.
Targets, completeness, and conduits
The proposed revascularization plan organized around its targets, completeness, and conduit considerations—without prescribing an operation.
What may still be missing
A practical view of incomplete imaging, testing, documentation, or questions to bring back to your treating clinicians.
Surgeon and center context
Procedure-specific experience, public outcomes, geography, and practical considerations when the care setting matters.
WHITEGLOVE Heart Team
The operating-room view and the cardiology view—on the same record set.
Every service level includes both independent reviews and both physician signatures. The physicians confer before the report is finalized.
Bypass targets · conduits · completeness · operative plan · surgical risk
Coronary anatomy · ischemia · PCI context · guideline-directed therapy · heart function
Ready for an independent read?
Put a cardiac surgeon and cardiologist on the same coronary record.
The $495 option includes both independent physician reviews and one co-signed written report. Live consultation is not included at this level.
How it works
From scattered records to one clear next conversation.
The 24-hour written-review clock starts only after all required records and imaging for your case have been received and confirmed complete.
- 01
Message us about the decision
Tell us what you were told, what is already scheduled, and what still feels unresolved. No referral or records are needed to begin.
- 02
We help assemble the required record
Upload what you have or authorize the records team to help gather the catheterization images and report, echocardiogram, notes, labs, testing, and proposed plan required for review.
- 03
Two physicians review independently
A cardiac surgeon and cardiologist examine the same record from their respective clinical perspectives, then confer.
- 04
Receive one co-signed report
Your WHITEGLOVE Insights™ report is delivered within 24 hours only after all required records and imaging have been received and confirmed complete.
Clinical rigor
Source-linked reasoning, not a generic answer.
2021 · ACC/AHA/SCAICoronary revascularization guideline: patient-centered Heart Team decisions2023 · MultisocietyChronic coronary disease guidance: medical therapy and revascularizationSociety of Thoracic SurgeonsAdult Cardiac Surgery Database operative risk calculator
Professional guidance and risk models inform—but do not replace—case-specific physician judgment. Model estimates have limitations and do not predict an individual outcome with certainty.
Start with the written review
One decision.
One clear starting point.
Every option begins with the same independent review by a cardiac surgeon and cardiologist. Choose live physician time only if you want it.
WHITEGLOVE Insights™
$495Independent review by both physicians and the co-signed written report.
WHITEGLOVE Consult
$995The written report plus a live consultation with one reviewing physician.
WHITEGLOVE Heart Team
$1,495The written report plus both reviewing physicians together on the consultation.
WHITEGLOVE Concierge
$2,495The Heart Team consultation plus concierge access until the day of surgery.
Direct-pay service. WHITEGLOVEMD does not submit insurance claims. No referral is required.
CABG second-opinion FAQ
Questions families ask before bypass surgery.
What is reviewed in a CABG second opinion?+
A cardiac surgeon and cardiologist review the records relevant to your decision, which may include the catheterization report and images, echocardiogram, ischemia testing, clinical notes, medications, laboratory results, prior cardiac procedures, and the proposed bypass plan. The final WHITEGLOVE Insights™ report organizes the current plan, reasonable alternatives when applicable, individual risk, missing information, and questions for your treating team.
Can the review compare bypass surgery with stents or guideline-directed medical therapy?+
Yes, when those paths are relevant to the documented anatomy and clinical situation. The report may compare CABG with PCI or stenting, guideline-directed medical therapy alone, or additional evaluation. Medical therapy and risk-factor management remain foundational whether or not revascularization is performed; medication changes stay with the treating clinicians.
What factors influence CABG versus PCI or stenting?+
The decision may be influenced by the pattern and complexity of coronary disease, left-main or multivessel involvement, diabetes, left-ventricular function, symptoms and ischemia, prior procedures, other health conditions, and patient preferences. The report places the documented factors in your case beside current guidance and evidence for discussion with your treating clinicians.
Does the report review the proposed bypass targets and grafts?+
The report can organize the documented target vessels, completeness of the proposed revascularization, and conduit considerations such as internal mammary, radial-artery, and vein grafts. It explains the relevant questions and uncertainties without prescribing a specific operation or replacing the surgeon responsible for your care.
How is my individual bypass-surgery risk assessed?+
The review considers the current STS Adult Cardiac Surgery Database operative-risk estimate when it applies and the required inputs are available. It identifies missing variables and places the estimate beside clinical details the model may not fully represent. Other scores are discussed only when they are already documented in the source record. Any estimate supports discussion; it does not predict an individual outcome with certainty.
Who reviews my CABG case?+
A cardiac surgeon and cardiologist independently review the same record set, then confer and co-sign one patient-facing WHITEGLOVE Insights™ report. Their two perspectives are included at every service level.
How much does a CABG second opinion cost?+
WHITEGLOVE Insights™ is $495 and includes the two independent physician reviews and co-signed written report; it does not include a live physician consultation. WHITEGLOVE Consult is $995 and adds a live consultation with one reviewing physician. WHITEGLOVE Heart Team is $1,495, and WHITEGLOVE Concierge is $2,495. WHITEGLOVEMD is a direct-pay service and does not submit insurance claims.
When does the 24-hour turnaround begin?+
The written report is delivered within 24 hours only after all required records and imaging have been received and confirmed complete. Time spent identifying, requesting, transferring, or collecting records and imaging is outside that window. The records team can help identify and gather what is needed with your authorization.
Do I need a referral or have to travel?+
No referral or travel is required. The medical-record review is completed remotely. You may choose the written review alone or a service level that also includes a live physician consultation.
What if bypass surgery is already scheduled?+
You can request a review after a surgery date has been set, but timing depends on how quickly the necessary records become available and how urgent your condition is. Continue following your treating team’s instructions, and do not delay urgent or time-sensitive care while waiting for a second-opinion service.
Does WHITEGLOVEMD replace my surgeon or cardiologist?+
No. WHITEGLOVEMD provides a limited-scope independent medical-record review. It does not provide emergency or ongoing treatment, order tests or medications, or replace the clinicians responsible for your care. The reviewing physicians’ role is defined in the consent and service terms.
The decision stays yours
Before bypass surgery, bring both sides of the coronary decision to the table.
Tell us what you were told, what is already scheduled, and what still feels unclear.
Our team calls within 2 business hours. During business hours, a same-day conversation with a cardiac surgeon or cardiologist may be arranged only when clinically appropriate and a physician is available.