When is a mitral valve second opinion useful?+
A second opinion can be useful when repair, replacement, TEER, or continued monitoring is being discussed and you want to understand the mechanism of regurgitation, the timing, repairability, alternative approaches, individual risk, or whether another cardiac problem changes the plan. It should not delay urgent or time-sensitive care directed by your treating team.
Can a mitral valve be repaired instead of replaced?+
Sometimes, but not every valve is durably repairable. The answer depends on the actual mechanism, leaflet and annular anatomy, calcification, tissue quality, prior procedures, and experience relevant to that lesion. The review organizes what the available imaging suggests, what remains uncertain, and why repair or replacement is being proposed without promising a repair result.
What is the difference between primary and secondary mitral regurgitation?+
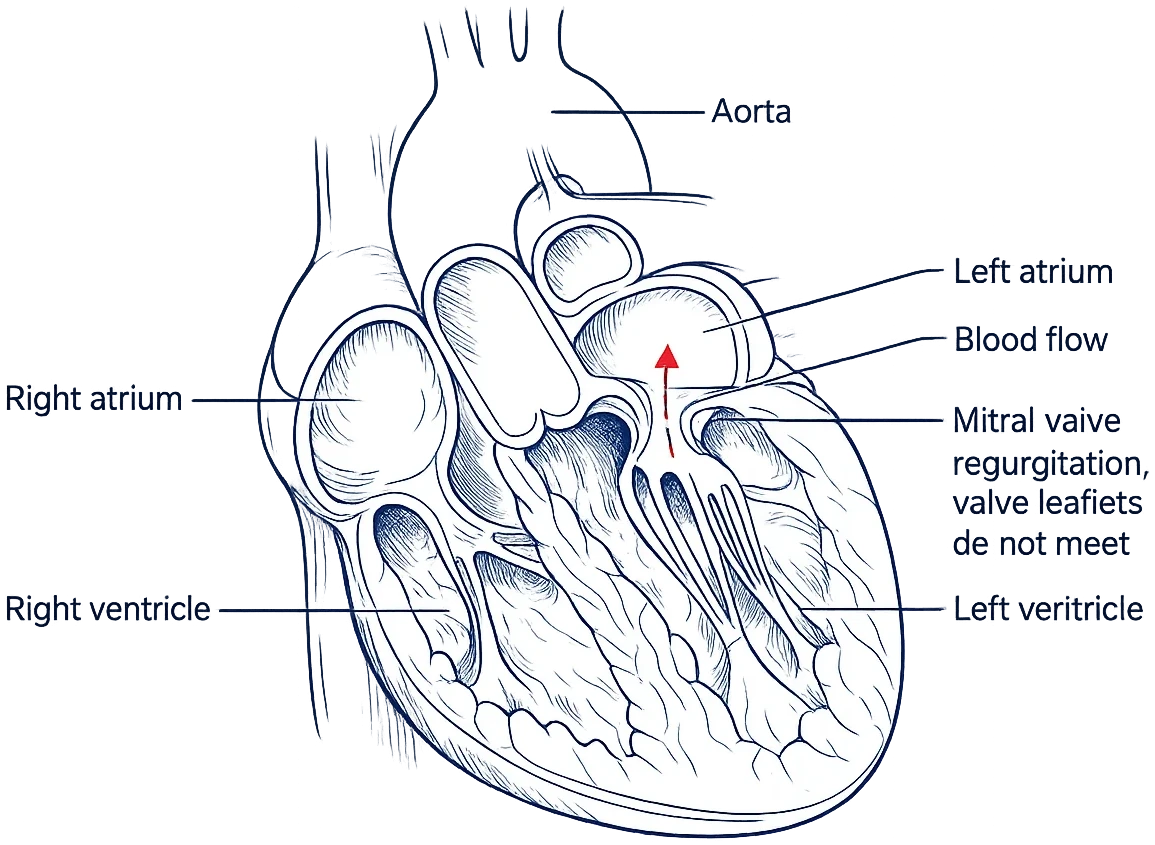
Primary mitral regurgitation begins with disease of the valve apparatus, such as prolapse or a flail leaflet. Secondary regurgitation occurs because changes in the ventricle or atrium prevent the leaflets from meeting normally. The distinction matters because the roles of repair, replacement, TEER, medical therapy, rhythm treatment, and monitoring can differ.
Could TEER, such as MitraClip, be an alternative to surgery?+
TEER may be reasonable for selected patients. In primary MR, candidacy generally includes symptoms, suitable anatomy, and high or prohibitive surgical risk. In secondary MR, persistent severe symptoms despite optimized guideline-directed heart-failure therapy and CRT when indicated are considered alongside ventricular status and other clinical and anatomic criteria. A catheter procedure is not automatically better or less appropriate than surgery; the comparison is case-specific.
Will the review compare mechanical and tissue valves if replacement is proposed?+
Yes, when replacement is a relevant option. The report can organize trade-offs involving durability, lifelong anticoagulation, bleeding and clotting considerations, lifestyle, pregnancy considerations when relevant, and possible future procedures. It does not prescribe a prosthesis; the final choice belongs with you and your treating physicians.
What records are needed for a mitral valve second opinion?+
The exact record depends on the decision. It commonly includes transthoracic echocardiogram images and reports, TEE images and report when performed or clinically relevant, catheterization or coronary assessment, clinical notes, laboratory results, medication history, rhythm information, and the proposed treatment plan. With your authorization, the records team can help identify, request, and organize what is needed.
Who reviews my mitral valve case?+
A cardiac surgeon and cardiologist independently review the same record set received and confirmed complete for the review, then confer and co-sign one WHITEGLOVE Insights™ report. Both perspectives are included at every service level.
How quickly is the written report delivered?+
The written report is delivered within 24 hours only after all required records and imaging have been received and confirmed complete. Time spent identifying, requesting, transferring, or collecting records and imaging is outside that 24-hour window.
How much does a mitral valve second opinion cost?+
WHITEGLOVE Insights™ is $495, WHITEGLOVE Consult is $995, WHITEGLOVE Heart Team is $1,495, and WHITEGLOVE Concierge is $2,495. Every option includes the two independent physician reviews and co-signed written report. The service is direct pay and WHITEGLOVEMD does not submit an insurance claim.
Does WHITEGLOVEMD replace my valve team?+
No. WHITEGLOVEMD provides independent educational decision support and medical-record review. It does not diagnose, prescribe, perform procedures, provide emergency care, or replace the physicians responsible for your treatment.